
Rheumatoid arthritis (RA) is the most common inflammatory rheumatic joint disease, affecting women 2-3 times more often than men. The exact interaction of immunological, hormonal and genetic factors has not yet been sufficiently researched. However, in order to enable improved, individualized medical care for our patients with inflammatory rheumatic diseases such as RA in the future, it is essential to take gender-specific or gender-dependent factors into account.
You can take the CME test in our learning platform after recommended review of the materials. Please click on the following button:
Rheumatoid arthritis (RA) is the most common inflammatory rheumatic joint disease, affecting women 2-3 times more often than men. RA is an autoimmune disease that generally affects more women than men. Men, on the other hand, suffer malignant diseases more frequently. The reasons for this so-called “gender bias” are manifold, including known differences in the immune systems of women and men, but hormonal (e.g. sex hormones) and genetic causes also play an important role [1]. The exact interaction of immunological, hormonal and genetic factors has not yet been sufficiently researched. Overall, research on gender-specific differences in rheumatology is still very limited. However, in order to enable improved, individualized medical care for our patients with inflammatory rheumatic diseases such as RA in the future, it is essential to take gender-specific or gender-dependent factors into account.
From the gender-dependent studies on RA to date, differences can be observed with regard to the course of the disease, the experience of the disease or the disease burden as well as comorbidities and the occurrence of cardiovascular events, the occurrence or distribution of autoantibodies as well as with regard to the utilization of the health care system, which are presented in the following text.
Course of the disease
The course of the disease is decisive for the long-term outcome of those affected. Early diagnosis and the earliest possible effective initiation of treatment with so-called DMARDs (disease-modifying antirheumatic drugs) prevents the occurrence of long-term damage, such as joint destruction and loss of function, and thus reduces long-term disability for those affected. Due to many modern treatment options (especially the use of biologics), RA patients are now treated according to the so-called “treat-to-target” (T2T) strategy – with the aim of achieving the best possible outcome of the disease [2].
In a Swedish study from 2004, a total of 844 patients (538 women) with early RA were included and prospectively examined over a period of 2 years with regard to gender-specific differences. The results show that women were significantly younger than men at the time of diagnosis (54.4 vs. 60.3 years old; p<0.001) – at age <40 years, the gender distribution was even 5:1 for women to men – and women also had lower median inflammation values: CRP 17 vs. 26 mg/l (p<0,001). The mean disease activity score DAS28 (Disease Activity Score28) of women was higher than that of men at diagnosis: 5.2 vs. 5.0 (p=0.02), and women also had a poorer functional score: HAQ(Health Assessment Questionnaire) scoreof 1.0 vs. 0.75 (p<0.001). After 2 years, women continued to have significantly higher disease activity on the DAS28 (3.6 vs. 3.1) and poorer functionality as measured by HAQ scores (0.5 vs. 0.25, both p<0.001). However, there were no differences in the X-ray findings (erosions using the Larsen score) between the two sexes. A gender-dependent (to the disadvantage of women) poorer treatment response, which is associated with persistently increased disease activity, is assumed to be a possible reason for the differences between the sexes [3].
Experience and burden of illness
Compared to men, women have an overall higher sensitivity to pain, which automatically results in higher pain scores from the questionnaires of women with RA. It is therefore not surprising that the symptoms reported by RA patients do not necessarily correlate with evidence of inflammation that can be objectified using functional MRI [4]. In addition, the DAS28 disease activity score is heavily weighted by the number of joints with pressure pain. Possible reasons for the increased pain and thus illness experience of female RA patients are that sex hormones generally influence pain transmission, modulation and perception, e.g. testosterone increases the pain threshold [5]. In addition to the influence of hormones, women have a greater number of pain receptors and a different expression of these receptors, e.g. in relation to opioid receptors [6]. Human genetic studies have also shown a gender-dependent involvement of certain genes in acute and chronic pain characteristics. In addition, it is important to note that immune cells and associated molecules, especially T cells, show qualitative sex differences in chronic pain [7]. In addition, differences in pain perception are most likely also influenced by external factors such as expectations, stereotypes, cultural differences, pain beliefs, previous pain experiences and environmental stress [8,9].
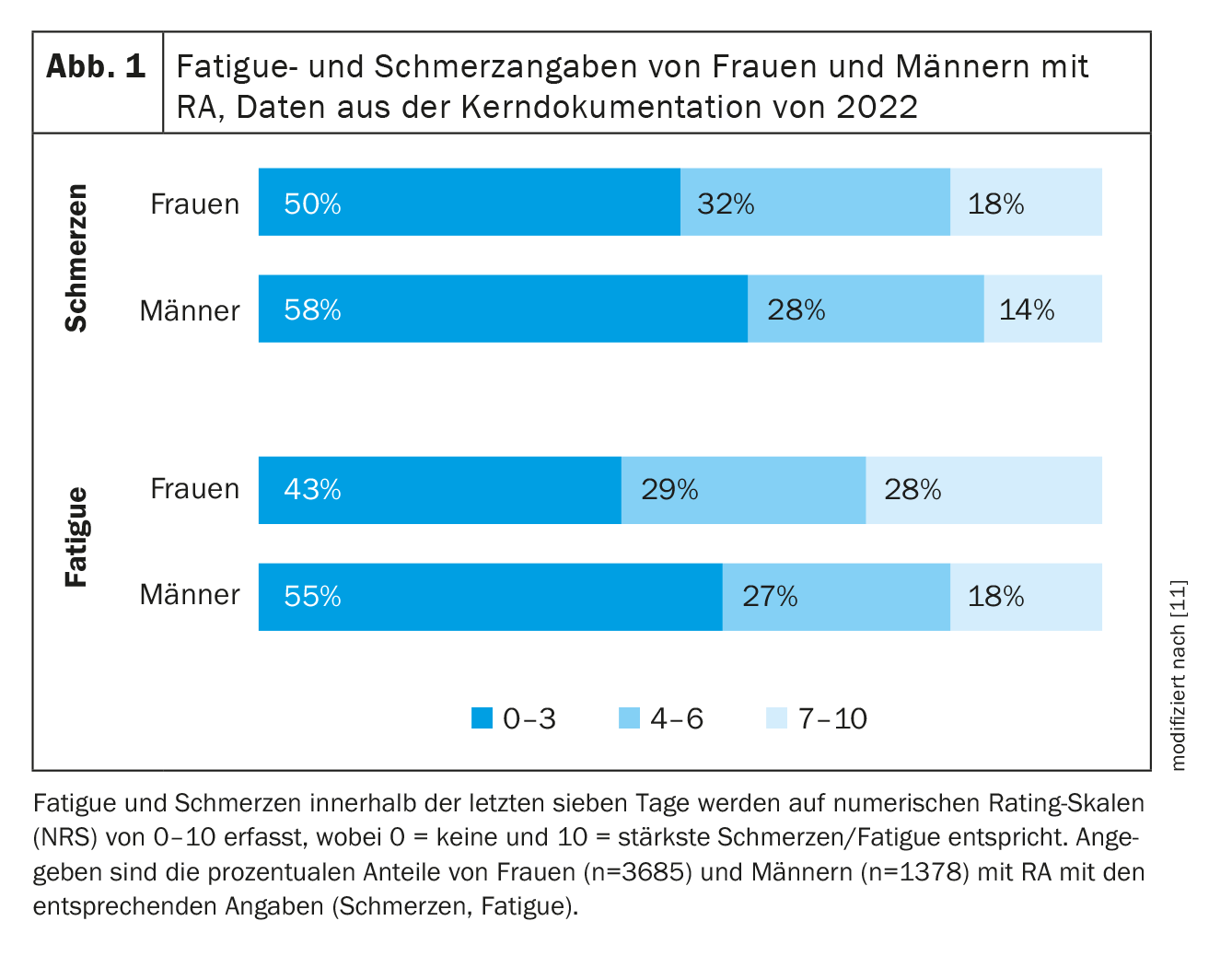
It is not only pain that plays a major role in how RA patients experience the disease and the burden of illness, but also fatigue symptoms, i.e. excessive tiredness. In a study on gender-specific differences in RA on fatigue symptoms, 228 women and men were included and examined with regard to possible influencing factors on fatigue symptoms. On days with an above-average number of positive events, the female RA patients included in the study were both less tired on the same day and more tired the next day (“hangover”), whereas this had no effect on the male patients. For both genders, days with an above-average number of negative events were associated with increased fatigue on the same day and the next day [10]. Current data from 3685 female and 1378 male RA patients from the core documentation of the regional cooperative rheumatism centers in Germany show higher fatigue and pain data in women compared to men. For example, 57% of women and 45% of men reported moderate to severe fatigue symptoms (Fig. 1) [11].
Comorbidities
In general, comorbidities not only influence the choice of anti-rheumatic therapy, but also the response to therapy and the further course of the disease. An analysis of health insurance data from Germany in 2015 showed that, in addition to cardiovascular risk factors, arthrosis (44%), depression (32%) and osteoporosis (26%) were the most common concomitant diagnoses in RA. While women were more likely to have depression, osteoporosis, osteoarthritis and hypothyroidism, men were more likely to have coronary heart disease, diabetes, cardiac arrhythmias and vascular disease (Fig. 2) [12].

In a review by Albrecht et al. from 2014 presented gender-specific aspects with regard to comorbidities in RA [13]. The main focus here was on controlling cardiovascular risk factors in men, but also on cardiovascular events as the most common cause of death in older women with RA. The need for osteoporosis prophylaxis also exists in men with RA and corresponding risks (e.g. glucocorticoid therapy). Hypothyroidism, which often occurs concomitantly in women, can be detected by checking the thyroid function.
Distribution of autoantibodies
In the majority of patients with RA, positive antibodies can be detected in the serum at the onset of the disease: Rheumatoid factors (RF) and/or antibodies against citrullinated peptides (ACPA, e.g. anti-CCP); these patients are then considered seropositive. Seropositivity for RF and/or ACPA is associated with an increased risk of erosiveness, i.e. these patients are more likely to have a joint-destructive disease course [14], in addition, ACPA-positive RA patients have an increased risk of developing interstitial lung disease (so-called RA-ILD) [15]. The male sex is also considered a risk factor for the development of RA-ILD [15].
In a Swedish study, the sera of 1600 patients (70% women) who developed RA within one year were examined for the positivity of anti-CCP2 antibodies and RF (IgA, IgG and IgM) [16]. 64% were anti-CCP2 positive, 43% were positive for RF-IgA, 33% for RF-IgG and 57% positive for IgM-RF. Women were more often RF-IgM positive and men more often RF-IgG/IgA positive. No gender differences were found for CCP2-AK positivity, but there was an age-dependent occurrence here (younger RA patients were more frequently CCP2 positive). These findings that ACPA are elevated in early RA – irrespective of gender – and that RF subclasses in favor of IgM are more likely to be found in women and IgA/IgA in men, should therefore be taken into account in the assessment of (early) antibody serology.
Utilization of the healthcare system
A recently published study, which included patients with RA (in addition to psoriatic arthritis and ankylosing spondylitis), investigated the impact of gender on healthcare utilization. In this Canadian cohort study, patients with the aforementioned inflammatory arthritis were analyzed three years before and three years after diagnosis with regard to the frequency of a medical consultation as well as laboratory and imaging examinations. The result for all three diseases mentioned was that women were more likely than men to present to a rheumatologist both before and after diagnosis – and also received more frequent laboratory and imaging examinations. Although the study confirms that women are more health-conscious, it also raises the question of why women are not diagnosed earlier with inflammatory arthritis, such as RA, which should lead to a better outcome. In future, gender-specific strategies should therefore be developed for both the early diagnosis and treatment of inflammatory arthritis in order to reduce the difference in disease progression between male and female patients with inflammatory arthralgias in the long term [17].
Take-Home-Messages
- Women and men with RA differ in many ways.
- From the manifestation to the course of the disease to the experience of the disease, there are many aspects that also influence the outcome of the disease.
- Knowledge of gender-specific influencing factors helps us to better assess the response to the various treatment options and to improve the individual care of women and men with RA.
Literature:
- Klein SL, Flanagan KL: Sex differences in immune responses. Nat Rev Immunol 2016; 16(10): 626-638; doi: 10.1038/nri.2016.90.
- Smolen JS, Landewé RBM, Bergstra SA, et al: EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis 2023; 82(1): 3-18; doi: 10.1136/ard-2022-223356.
- Tengstrand B, Ahlmén M, Hafström I: The influence of sex on rheumatoid arthritis: a prospective study of onset and outcome after 2 years. J Rheumatol 2004; 31(2): 214-222.
- Schrepf A, Kaplan CM, Ichesco E, et al: A multi-modal MRI study of the central response to inflammation in rheumatoid arthritis. Nat Commun 2018; 9(1): 2243.
- Aloisi AM, Affaitati G, Ceccarelli I, et al: Estradiol and testosterone differently affect visceral pain-related behavioral responses in male and female rats. Eur J Pain 2010; 14(6): 602-607.
- Niesters M, Dahan A, Kest B, et al: Do sex differences exist in opioid analgesia? A systematic review and meta-analysis of human experimental and clinical studies. Pain 2010; 151(1): 61-68.
- Mogil JS: Qualitative sex differences in pain processing: emerging evidence of a biased literature. Nat Rev Neurosci 2020; 21: 353-365.
- Gazerani P, Aloisi AM, Ueda H: Editorial: Differences in Pain Biology, Perception, and Coping Strategies: Towards Sex and Gender Specific Treatments. Front Neurosci 2021; 15: 697285.
- Keogh E: The gender context of pain. Health Psychol Rev 2021; 15(3): 454-481.
- Davis MC, Okun MA, Kruszewski D, et al: Sex differences in the relations of positive and negative daily events and fatigue in adults with rheumatoid arthritis. J Pain 2010; 11(12): 1338-1347.
- Thiele K, Albrecht K, Alexander T, et al: Core documentation of the regional cooperative rheumatology centers – care trends 2024; doi: 10.17169/refubium-41983.
- Luque Ramos A, Redeker I, Hoffmann F, et al: Comorbidities in Patients with Rheumatoid Arthritis and Their Association with Patient-reported Outcomes: Results of Claims Data Linked to Questionnaire Survey. J Rheumatol 2019; 46(6): 564-571; doi: 10.3899/jrheum.180668.
- Albrecht K: Gender-specific differences in comorbidity in rheumatoid arthritis [Gender-specific differences in comorbidities of rheumatoid arthritis]. Z Rheumatol 2014; 73(7): 607-614.
- Arnason JA, Jónsson T, Brekkan A, et al: Relation between bone erosions and rheumatoid factor isotypes. Ann Rheum Dis 1987; 46(5): 380-384.
- Fazeli MS, Khaychuk V, Wittstock K, et al: Rheumatoid arthritis-associated interstitial lung disease: epidemiology, risk/prognostic factors, and treatment landscape. Clin Exp Rheumatol 2021; 39(5): 1108–1118.
- Pertsinidou E, Manivel VA, Westerlind H, et al: Rheumatoid arthritis autoantibodies and their association with age and sex. Clin Exp Rheumatol 2021; 39(4): 879-882.
- Tarannum S, Widdifield J, Wu CF, et al: Understanding sex-related differences in healthcare utilization among patients with inflammatory arthritis: a population-based study. Ann Rheum Dis 2023; 82(2): 283-291.
InFo RHEUMATOLOGIE 2024; 6(1): 6–8









