Dilatation of the ascending aorta above 40 mm (descending aorta above 50 mm and abdominal aorta above 40 mm) requires control. There are no restrictions for patients with diameters below 40 mm. From 40 mm no contact sports or sports with strong isometric loads should be performed, from 45-50 mm no sports with sudden accelerations and decelerations. Any sports activity should be suspended in the presence of aneurysms >55-60 mm. After elective aortic interventions without remaining segments with dilatation, there are few restrictions on exercise. After dissections, exercise should not be performed for the first six months, except in the context of rehabilitation and mild endurance exercises under strict blood pressure control. No competitive sports in persistent aortic problems.
“There is no disease more conducive to clinical humility than aneurysm of the aorta.” (Sir William Osler)
Every day you can read about new trend sports like ZUMBA, Kettlebell or High Intensity Training. The traditional sports such as skiing and cycling to swinging are pleased with increasing numbers of young people. But what are the effects of these forms of stress on the human aorta, which is so vital? And which sports are suitable for patients with thoracic aneurysms?
The current guidelines are not as specific in this regard as one would like. Therefore, the following recommendations are based on the experience of the many patients seen in our aortic consultation. This consultation was established almost 20 years ago at the Clinic for Cardiovascular Surgery of the Inselspital and can draw on clinical examinations and imaging procedures in more than 3000 patients, with operated and non-operated pathologies in the thoracic and abdominal aorta.
In the general population, the prevalence of thoracic aneurysms is approximately 1%. Arterial hypertension is one of the most common risk factors, but bicuspid aortic valve or monogenetic causes such as Marfan, Loeys-Dietz, or Ehlers-Danlos syndrome are also included. Due to the widespread use of imaging techniques, the number of those patients in whom aortic dilatation is detected but surgical treatment is not yet indicated is growing. Particularly in this group of patients, the question arises as to which sporting activities may still be undertaken without risk.
Should patients with aortic disease exercise at all?
Dilatations of the aorta present the clinician with major diagnostic and treatment challenges due to the often clinically silent course for years until the onset of sometimes life-threatening complications. There is no question that moderate aerobic exercise significantly reduces the risk of dying from cardiovascular disease. But how to deal with the desire to exercise in patients with diseases of the aorta? Although differentiated, evidence-based recommendations are lacking in many cases, differences between different patient populations must certainly be considered here.
Definition of aortic aneurysms
An aneurysm is a dilation of the vessel diameter by more than 1.5 times the adjacent normal vessel diameter. Of course, this depends on age, gender, height and weight. Smaller enlargements are called ectasia. As a rule of thumb for the clinician, dilatation of the ascending aorta above 40 mm is certainly in need of control and surgical intervention should be considered in most patient groups above 50 mm. In the descending aorta, the intervention limit is 55 to a maximum of 60 mm; in the abdominal aorta, it is 45 mm.
Sport with dilated aorta
Due to the increasing prevalence of imaging modalities, the number of those patients in whom aortic dilatation is detected but surgical treatment is not yet indicated is growing. Particularly in this group of patients, the question arises as to which sporting activities are still possible without risk. The current guidelines [1,2] are not very specific and only state that competitive sports or sports with potential (violent) physical contact should be avoided in patients with an enlarged aorta.
In general, we see no need for restrictions in patients with diameters below 40 mm. From a diameter of 40 mm in the area of the ascending aorta, we recommend refraining from contact sports as well as sports with strong isometric loads. From 45-50 mm, we additionally recommend not to practice other sports with sudden accelerations and decelerations, such as skiing, volleyball or even golf. We only recommend stopping any sporting activity in the case of aneurysms >50-55 mm, which should be treated surgically in the relatively short term anyway.
Sport after elective aortic surgery
In patients after elective aortic surgery, the extent of surgical intervention and the question of remaining dilated sections of the aorta must certainly be discussed. For example, if the entire diseased segment could be removed in an isolated replacement of the ascending aorta, most sports can be resumed after complete healing of the sternotomy, usually after three months. According to current guidelines, however, the practice of competitive sports must be discouraged here as well.
Sport after aortic dissection
Patients with condition after operated acute aortic dissection Stanford type A, but also patients with conservatively treated aortic dissection type B, are at risk of increasing aneurysmal dilation or even rupture. The recommendations here are to aim for a target blood pressure of less than 120/80 mg. We recommend that patients avoid lifting and carrying loads over 5 kg for the first six months and refrain from sports. Exceptions are physical activity in the context of rehabilitation measures and mild endurance activities (running, swimming, cycling) under control of heart rate and blood pressure.
The further procedure depends on the clinical and radiological course. In patients after or with aortic dissection, a rapid increase in dP/dt should be avoided at all costs, so that they should be advised against sports with isometric loads even in the long term. For subjective assessment, we tell patients to avoid lifting a weight or activities that require the patient to perform a Valsalva maneuver.
Sports in children with aortic diseases and in patients with connective tissue diseases.
The data situation in children is even more sparse than in adults, and guidelines are of course sometimes difficult to enforce in children. There is a tendency for parents, teachers, and even pediatricians to be rather overprotective, and so there is a risk that the child will be excluded from socially important activities. In our practice, we are therefore relatively liberal with regard to sports activities. Often, many problems can be avoided by choosing the right sport in advance. Contact sports such as judo, karate, swinging or ice hockey and sports with high isometric loads must be discouraged. If dissection has occurred, which is very rare in childhood, the stricter guidelines already mentioned apply.
In patients with connective tissue diseases, similar guidelines apply in principle as in patients without a confirmed (monogenetic) cause for aortic aneurysms. However, in patients with Marfan syndrome, the skeletal and muscular components of the disease must also be considered. In these patients, we aim for elective aortic root replacement as early as 45 mm, because at this diameter the likelihood of preserving the native aortic valve (within the dilated aortic root) is much higher. In patients with Loeys-Dietz syndrome, which is characterized by aneurysms, tortuous vessels, and a bifid uvula, aortic diameter as small as 30 mm in children and as large as 40 mm in adults must be considered. mm, intervention should be considered, as this patient group is at high risk for early dissection (even with smaller diameters).
Competitive sports as a risk factor
Sport under competitive conditions is in itself a risk for an event in terms of aortic dissection or rupture. It is part of the business that athletes push or exceed their limits in a competition. This can only be reconciled with the demands of controlled blood pressure, low dP/dt or always controlled movement in very few sports.
Many sports are already eliminated because of the isometric component. Thus, systolic values of up to 300 mmHg are reached during weight lifting. Sports with strong accelerations and decelerations, such as volleyball or competitive skiing, are also certainly unsuitable. Due to rapid rotational movements, sports such as basketball, tennis and golf are also discouraged as competitive sports. It should be noted in patients who do strength training that the use of artificial growth hormones and anabolic steroids also poses a risk (additional increase in blood pressure, sodium retention, direct effects on tissues) and must be absolutely refrained from.
Literature:
- Hiratzka LF, et al: ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease. Circulation 2010; 121: 266-369.
- Erbel R, et al: 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology. Eur Heart J 2014; 35: 2873-2926.
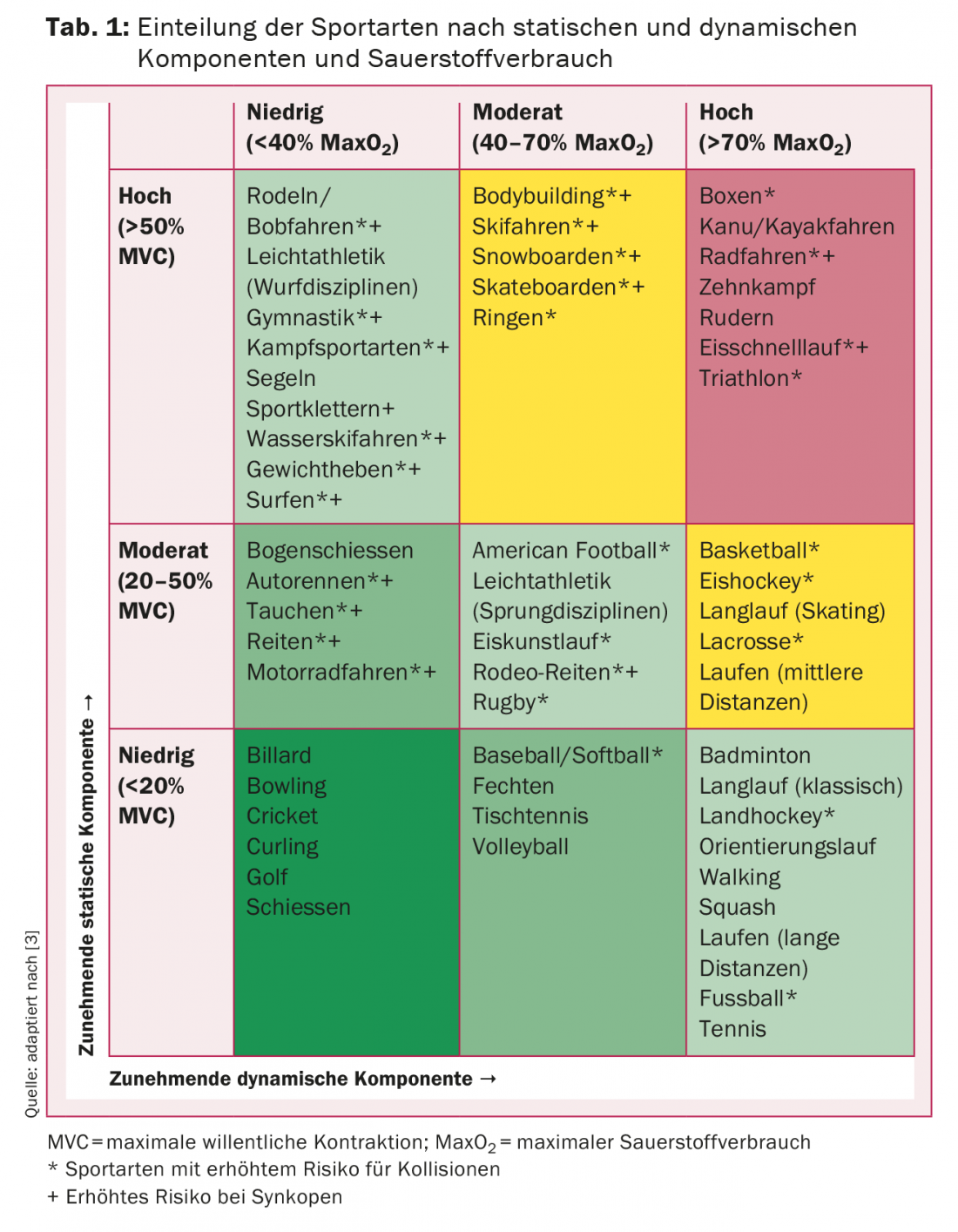
- Mitchell J, et al: 36th Bethesda Conference – Task Force 8: Classification of sports. J Am Coll Cardiol 2005; 45(8): 1364-1367. doi:10.1016/j.jacc.2005.02.015.
CARDIOVASC 2015; 14(2): 3-5