
On the occasion of the 3rd Swiss Life-Workshop Chemical Peeling, Oliver Ph. Kreyden, MD, summarized the most important points that determine the success of chemical peelings. As the initiator of the workshop, he demonstrated to the participants during a lecture and with live treatments how the substances differ, which technique they require and for which indications they are used. In the following interview, Dr. Oliver Kreyden provides information about the factors that must be taken into account in any peeling and explains which aspect is unfortunately often forgotten in aesthetic dermatology.
Dr. Kreyden, what did you primarily want to convey to the participants of the workshop?
Kreyden, MD:
That it is very, very important to make a diagnosis, also in aesthetic dermatology. Unfortunately, it happens again and again that doctors do not treat what would be necessary in the patient, but they treat according to what they can. And this is where the workshop came in.
How do you go about clarifying a patient’s needs?
For the diagnosis you have to analyze the patient’s face and find out where the problem is in the first place. It’s about recognizing the connections. Then it is necessary to weigh the basic treatment options against each other. The principle is relatively simple: botulinum toxin is used for mimic wrinkles, fillers are used for volume deficiencies, and chemical peels are used for structural changes in the skin.

Can you give a concrete example of this?
A patient comes into the practice and would like to have her nasolabial fold filled. However, in this situation, augmentation of the wrinkle itself does little to nothing. Rather, the cause of the wrinkle must be treated. And in this case, it is a lack of volume in the midface. The skin sags against gravity and this is how the nasolabial fold is formed. My credo is: Never treat the wrinkle itself, but always its cause!
When to use which chemical peel to achieve the best results?
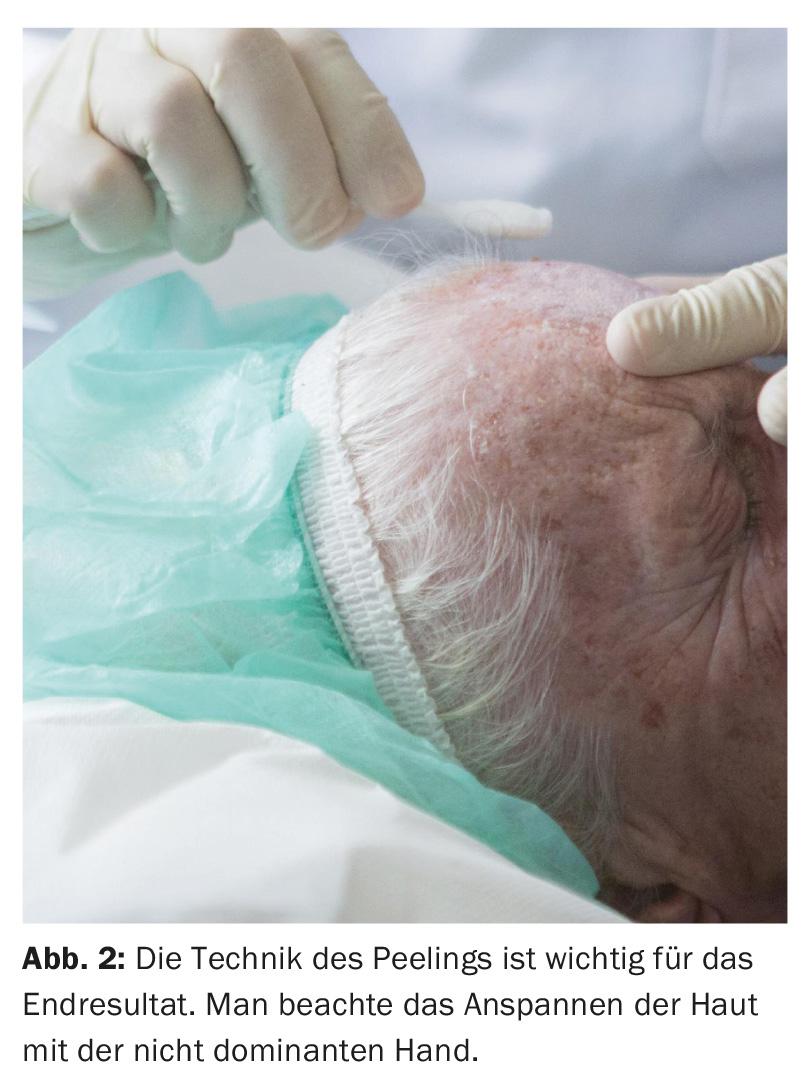
For superficial pigmentary changes such as lentigines, it is a superficial peel; for smile lines, which are already a structural problem of the skin, a medium-depth peel is indicated; and for deep wrinkles, it needs a deep peel. Again, of course, it is critical that doctors know what they are doing. With medium and deep peels, there is a risk of scars and it takes a lot of experience how to apply a solution. Technology plays a very important role here.
How do the peelings differ in their effect?
The superficial substances such as fruit acids, glycolic acids, salicylic acids cause irritation of the skin. You leave the pH of the skin as low as possible and leave the substance as long as possible, that is, for minutes. The result is moderate and in case of pigmentary changes the treatment already reaches its limits. TCA and phenol, on the other hand, do not function with irritation; they cause protein denaturation. The proteins are destroyed and the so-called frost forms on the tissue. The deeper the peeling, the stronger the frost. This is a process that cannot be reversed.
What should be considered when selecting a patient for a peel?
With a peel that causes structural changes, we are in a realm comparable to surgery. And patients usually don’t know that. They have little idea of what lies ahead. That’s why it needs very careful education. Often the first question is: How long does the effect last? Then I explain that the skin is treated so that it regenerates from the inside and therefore the effect is permanent.
Due to the violent reaction during a peel, not every patient is suitable for this treatment. The most important difference between lasers and peels is that the latter entails a very long inflammation period. With phenol, the face is subsequently very red for six to twelve weeks. The inflammation ensures that tight collagen fibers are formed again instead of elastic fibers, which results in an improvement of the overall skin appearance.
How do you explain to patients what’s coming up?
During the preliminary consultation, I show pictures of freshly treated patients and explain the stages of healing. In the preliminary information, nothing may be glossed over with regard to reaction. I would like to emphasize again, it takes a lot of education, you have to prepare the patients carefully for what to expect. Afterwards, patients go home and think about whether they really want this treatment. If they decide to do so, another hour-long consultation follows, in which I explain the treatment process in detail. After that, depending on the treatment, the patient makes another appointment with the anesthesiologist.

When do you work with an anesthesiologist?
In the case of a deep peel, it is imperative that the attending physician include a local anesthesiologist. It needs anesthesia because the pain of phenol treatment is very severe. Anesthesia also requires careful explanation and appropriate preliminary examinations. The higher the concentration, the deeper the solution penetrates and the stronger the pain, even after the treatment. With trichloroacetic acid (TCA), they subside after about half an hour; with phenol, they can last for hours.
What must be considered for the first time after treatment?
Patients are affected for weeks. They do not feel ill, but their appearance is severely affected. This is the case with deep peels, but also medium depth peels. And that is why so-called soft factors play an important role and must be taken into account accordingly. For example, whether the patient lives alone, whether and how he is supported in organizing everyday life. Sometimes it is small things that have a big meaning and these also need to be clarified beforehand.
You offer a new combination treatment in your practice, the photo peel. What are the advantages of this method?
I use the photo peeling for pigmentation on the face, hands and décolleté. With laser, results were below expectations, especially in the treatment of hyperpigmentation. Therefore, I proceeded to apply peels. In the area of the hands and décolleté, peelings are limited to superficial peelings with a maximum of TCA 25% with a correspondingly limited effect due to the reduced follicle density (regeneration).
The principle of photo-peeling is now to treat two superficial lesions of the same target structure with two different systems. First I do the laser treatment, which causes initial damage, and then double up with a 15% TCA solution. This way I achieve a multiplication of the effect with two superficial substances and the risk remains low because I can work with a superficial peeling.
Dr. Kreyden, thank you very much for this interview.
DERMATOLOGIE PRAXIS 2016; 26(6): 26-28









