At a DESO advanced training course in St. Gallen, Prof. Volker Heinemann, MD, Munich, and Prof. Werner Scheithauer, MD, Vienna, led a discussion on the use of first-line antiangiogenic therapies. The high age at diagnosis (80-84 years according to the Dutch Cancer Registry) of colorectal cancer (mCRC) is an important aspect in this question.
(dk) The FIRE-3 trial provides important arguments in the question of first-line antiangiogenic therapy in metastatic colorectal cancer (mCRC), although the data are not yet strong enough to bring about a change in clinical practice.
In this context, Prof. Dr. med. Volker Heinemann, Munich, emphasized the importance of molecular pathological KRAS mutation testing as the most important innovation in the therapy of metastatic colorectal cancer. For example, recent analyses confirmed that colorectal cancer patients with metastases have a significant survival advantage if their tumor cells contain a wild-type RAS gene without genetic alterations and they receive anti-EGFR therapy in addition to chemotherapy. “FIRE-3 compares a therapy that inhibits tumor-associated vascularization of the tumor with an anti-EGFR treatment that stops uncontrolled cell growth in the tumor,” explained Prof. Heinemann in his role as principal investigator of the Comprehensive Cancer Center at Ludwig Maximilian University in Munich. The result of the KRAS test should be used in the decision for first-line therapy in any patient with metastatic colorectal cancer. For patients with RAS wild-type status, the results of the FIRE-3 trial are encouraging, whereas for patients with a RAS mutation, these are much less certain. This affects 50% of all patients with metastatic colorectal cancer, according to Prof. Heinemann. For this reason, further studies are needed to achieve optimal therapy. He further emphasized the relevance of first-line therapy, as its response is critical to overall survival. Therefore, he advocates giving cetuximab directly to wild-type patients.

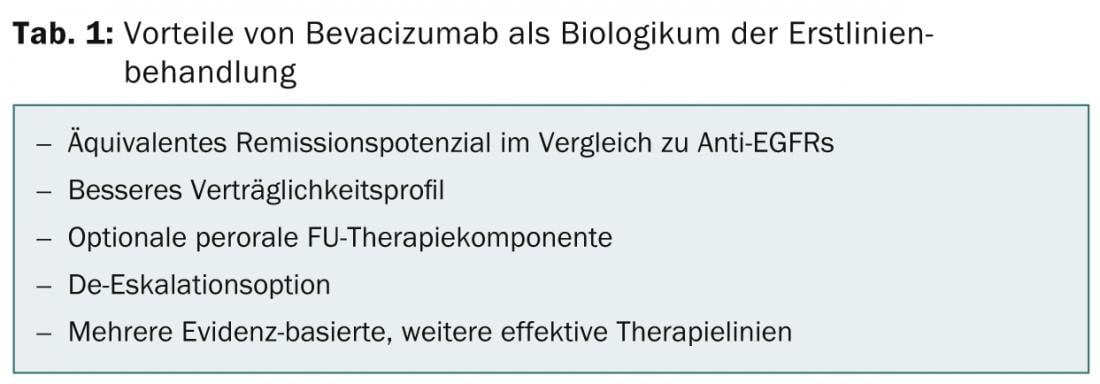
Prof. Werner Scheithauer, MD, Vienna, argued, “In disease dissemination, indolent disease, and elderly comorbid patients, sequential therapy with FU ± bevacizumab should be the primary approach.” At the same time, he would like to see a randomized phase III trial in RAS wild-type patients (standard vs. X + cetuximab). In mCRC ± RAS wild-type, bevacizumab offers a number of advantages as a frontline biologic (Table 1) if downsizing or at least averting progression were the primary therapeutic goal.
According to Prof. Scheithauer, FIRE-3 data do not yet carry the weight to change current clinical practice. Too many questions remain unanswered, such as those about bias, chance, and clinical reality. The data from CALGB-80405 could answer a few things here. In the positive case, Prof. Scheithauer would also give his consent for all, RAS mutants excluded, to be provided with anti-EGFR therapy.
Source: 24th Physician Continuing Education Course in Clinical Oncology, February 20-22, 2014, St. Gallen, Switzerland.
InFo Oncology & Hematology 2014; 2(5): 35-36.