Renal cell carcinoma tends to be one of the rarer malignant tumors in adults. In terms of drug treatment options, however, this tumor entity has undergone more rapid change in recent years than almost any other malignant disease. Meanwhile, the focus is not only on targeted therapy in advanced renal cell carcinoma, but also on combination treatments.
Kidney cancer is the third most common urologic cancer. Every year, nearly 1000 people in Switzerland develop a malignant renal tumor [1]. This corresponds to around 2% of all solid malignant tumors. Histologically, the majority of tumors are clear cell renal carcinomas, which – depending on the subtype – have a slightly better prognosis than non-clear cell renal cancer [2,3].
In the advanced stage, however, the prognosis is unfavorable for most of those affected: three quarters of them have a medium to high risk of the disease not coming to a halt [4]. However, the therapeutic landscape for metastatic renal cell carcinoma has changed significantly as a result of numerous new approvals. Targeted therapies were joined by immune checkpoint inhibitors, which can now also be used in combination [5].
Curative treatment possible at an early stage
Nevertheless, the most effective causal and only curative therapy is and remains surgery. A radical or partial nephrectomy can be performed. In partial nephrectomy, as much functioning kidney tissue as possible is preserved, as postoperative renal insufficiency is a negative prognostic factor. However, their success in stage T2 depends on careful patient selection and surgical expertise. In addition, at later stages, surgery is usually only advisable in combination with other treatment measures. Targeted combination therapies are then primarily used.
Targeted treatment management
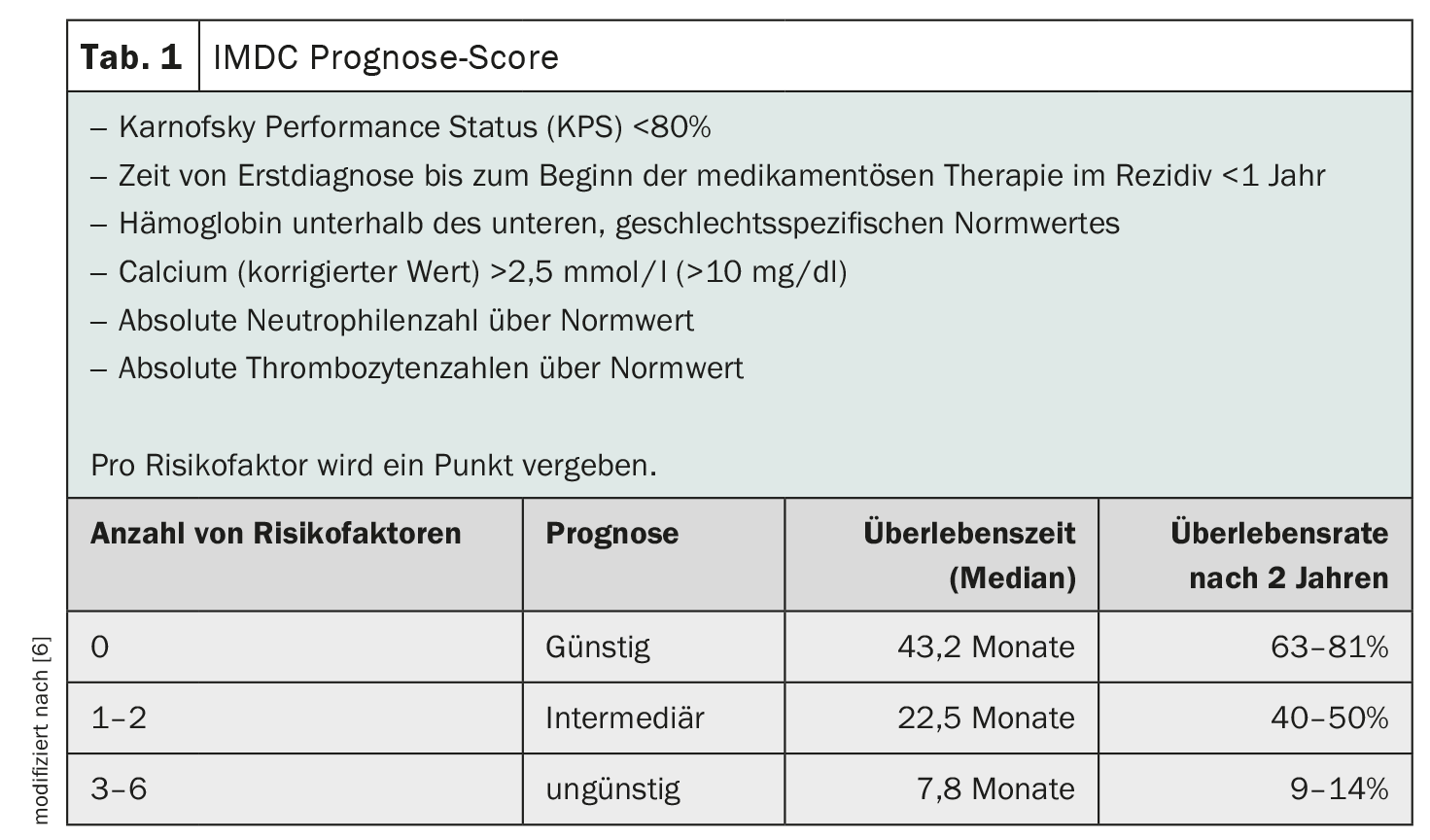
Targeted therapy with tyrosine kinase inhibitors, mTOR inhibitors or antibodies has become established in recent years. Inhibition of the VEGFR (vascular endothelial growth factor receptor) in particular is the standard option for patients with a favorable prognosis whose tumors could not be operated on or in whom metastases have formed [6] (Table 1) .
The first checkpoint inhibitor, which targets the surface protein PD-1, was then approved as a second-line therapy following the failure of a previous therapy. Dual immune checkpoint blockade is now also possible in earlier use. The combination therapy of the checkpoint inhibitor nivolumab with the antibody ipilimumab directed against CTLA-4 was approved. Compared with targeted therapy, dual checkpoint blockade shows advantages in patients with intermediate or unfavorable baseline risk.
At 18 months, 75% of those affected were still alive and median overall survival was not achieved during the study observation period. In 9% of those treated with immunotherapy, the disease responded completely to treatment, meaning that the tumor was initially no longer detectable after therapy [4]. However, the chance of achieving an optimal response and a long-lasting remission with the new therapeutics is accompanied by a high rate of side effects. Their treatment requires a well-coordinated interdisciplinary treatment team [5].
Combination therapies improve prognosis
Another way of immuno-oncological treatment of kidney cancer is to combine the proven targeted substances with checkpoint inhibitors. Combinations of, for example, the tyrosine kinase inhibitor axitinib with pembrolizumab (anti-PD-1 antibody) or axitinib with the anti-PD-L1 antibody avelumab are currently available. Pembrolizumab together with lenvatinib and nivolumab in combination with cabozantinib can also be used in advanced or metastatic renal cell carcinoma. If combination therapies cannot be used, monotherapy with cabozantinib or sunitinib, among others, can be used.
Literature:
- www.krebsliga.ch/ueber-krebs/zahlen-fakten/-dl-/fileadmin/downloads/sheets/zahlen-krebs-in-der-schweiz.pdf (last accessed on 23.04.2024)
- www.onkopedia.com/de/onkopedia/guidelines/nierenzellkarzinom-hypernephrom/@@guideline/html/index.html (last accessed on 23.04.2024)
- www.krebsgesellschaft.de/basis-informationen-krebs/krebsarten/nierenkrebs.html (last accessed on 23.04.2024)
- Motzer RJ, Nizar M, Tannier MD, et al: Nivolumab plus ipilimumab versus sunitinib in advanced renal cell carcinoma. N Engl J Med 2018; 378: 1277-1290
- Zschäbitz S, Ivanyi P, Delecluse S. Revolution in the systemic therapy of metastatic renal cell carcinoma. The Nephrologist 2020; 15: 12-19
- Ivanyi P, Grünwald V: Systems therapy of renal cell carcinoma. Oncologist 2019; 25: 517-522
- Heng DYC, Xie W, Regan MM, et al: External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol 2013; 14: 141-148.
InFo ONCOLOGY & HEMATOLOGY 2024; 12(2): 34







