
Hearing aids are the most common type of instrumental therapy for hearing loss. They can improve hearing and speech understanding. In very severe cases and complete deafness, cochlear implants are used. They take over the function of the inner ear.
The results of various studies show that in industrialized countries about 10% of the total population is affected by significant bilateral hearing loss [1,2]. The distribution is strongly age-dependent: While about 0.1% have an irreversible hearing impairment at birth [3], more than 30% of people over 65 years of age are affected [1,2].
Hearing loss in childhood and in adulthood
Childhood and adult hearing loss differ in several ways.
Especially in preschool age, transient conductive hearing loss due to chronic or even acute middle ear ventilation disorders predominates. In most children, this problem grows by the age of about five. However, in about one in 1000 children, a significant, bilateral and permanent sensorineural hearing loss is already present at birth, for which the only known treatment is the provision of hearing aids. The causes of these hearing disorders are manifold and by far cannot always be determined. They include, for example, genetic factors, maternal infections during pregnancy, neonatal icterus, perinatal infections of the child, and many other reasons.
Hearing disorders are less common in childhood than in adults, but are significant because of their impact on language acquisition, school, and education. Their correct detection and their therapy is the task of specialized departments at larger center hospitals. Newborn hearing screening [3] now allows early detection, so that the target hearing aid fitting is usually realistic by six months of age.
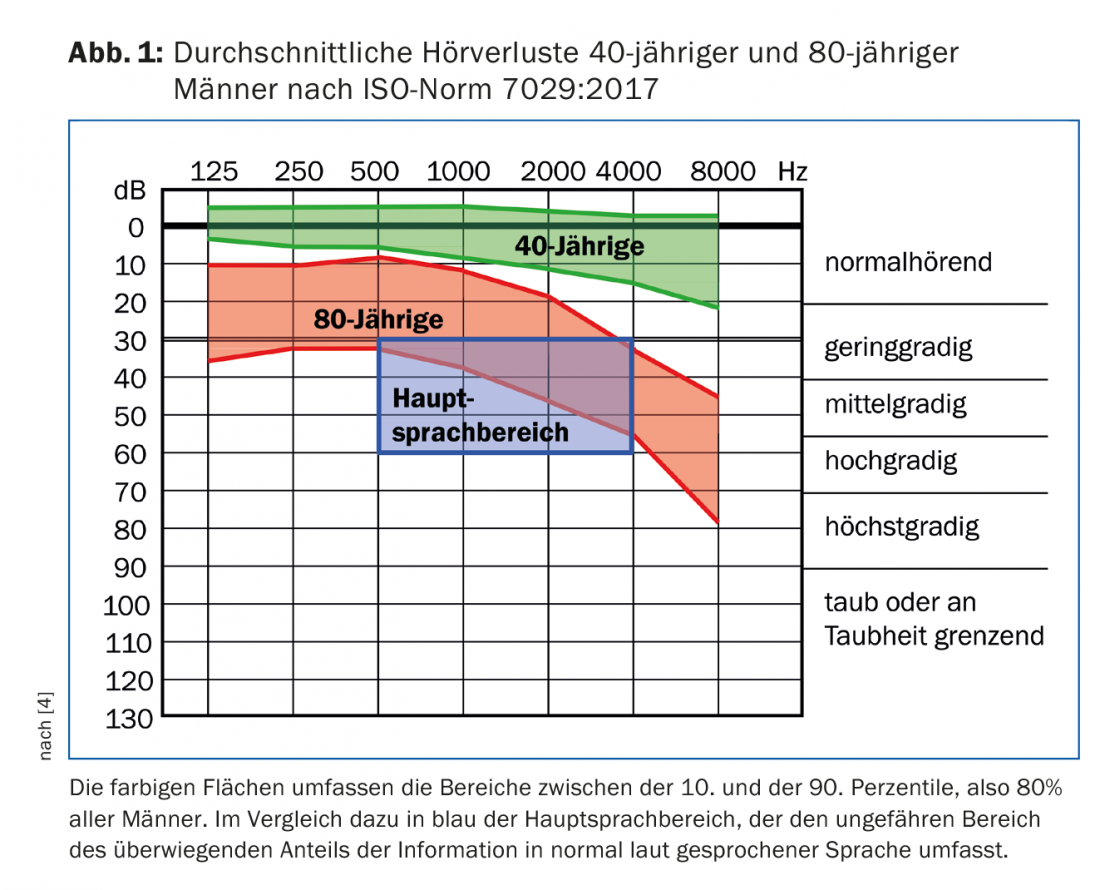
Causes of hearing loss that first manifest in adulthood are also diverse and include entities as varied as presbycusis, hearing loss, Meniere’s disease, otosclerosis, traumatic brain injury, bacterial meningitis, chronic middle ear infections, and acoustic trauma. In terms of numbers, however, presbycusis clearly predominates among adults. This is also evident from the progression of expected hearing thresholds as a function of age. Figure 1 shows the hearing thresholds of 40- and 80-year-old men according to the recently updated ISO 7029 standard [4]. With increasing age, hearing in the higher frequency range in particular deteriorates. Men are affected somewhat more strongly and somewhat earlier than women, but the difference accounts for only a few dB on average, while the individual and also interfamilial variability is much greater. Figure 1 additionally shows the approximate range in which normally loud speech contains the most information. Hearing loss, in which the higher frequencies are particularly affected, manifests itself in everyday life primarily through poor speech comprehension in noise. This can lead to social withdrawal by avoiding occasions such as parties or going to restaurants, where background noise is the norm. As Figure 1 shows, however, lower frequencies are also affected in age-related hearing loss, albeit to a lesser extent.
Normal sound transmission from the outer ear to the oval window is mechanical. In cases of hearing loss that is either purely or predominantly middle ear or outer ear related, the possibility of surgical remediation is usually explored first. Depending on the underlying pathology, hearing improvement may be achieved by, for example, eardrum closure or surgical restoration of sound transmission through the middle ear by stapedotomy.
Apparative therapy of hearing loss
For many hearing impairments, especially those caused by the inner ear, hearing aids are the treatment of choice. This applies to both children and adults.
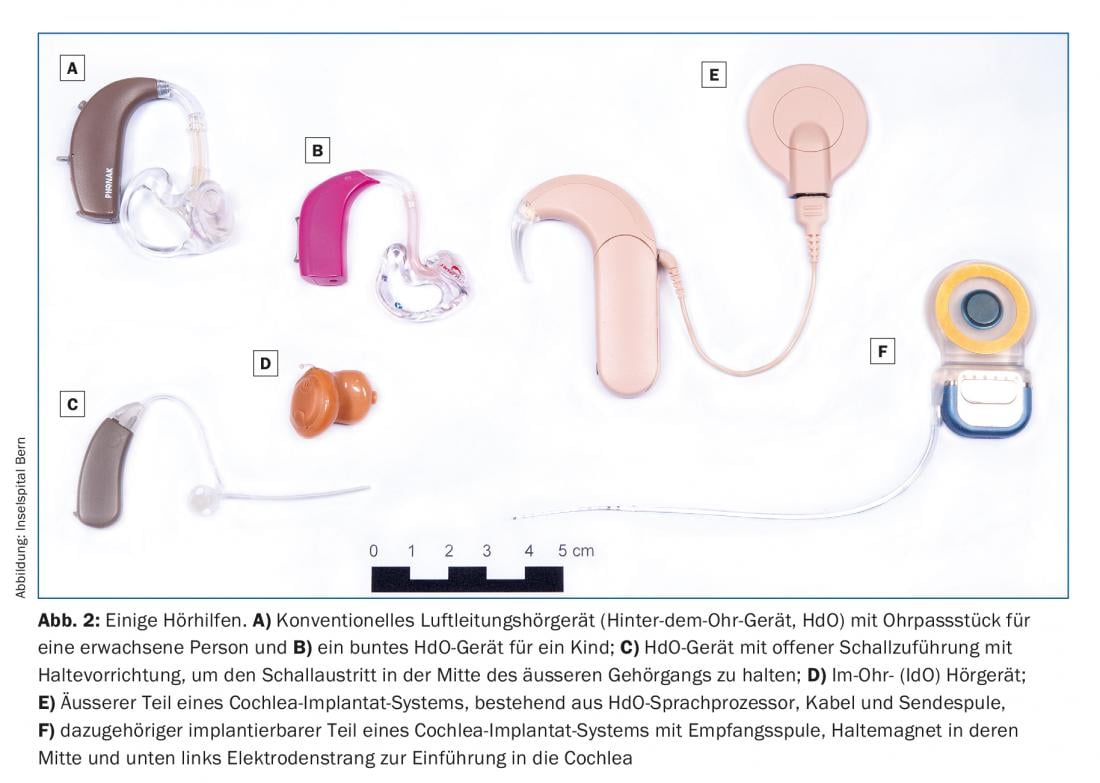
The most common hearing aid by a large margin is the conventional hearing aid (or air conduction hearing aid). Figure 2 shows some examples. Behind-the-ear (BTE) hearing aids with a custom-made earmold (Fig. 2A and B) are suitable for children and adults with mild to severe hearing loss. Hearing aids with open sound feed (Fig. 2C) and in-the-ear hearing aids (ITE, Fig. 2D) are not suitable for pronounced hearing losses due to the higher feedback tendency and are also not suitable for children because the auditory canal is not yet fully developed.
The main function of hearing aids is to amplify the incident sound in those frequency ranges where a hearing impairment is present. In addition, modern hearing aids reduce gain at higher input levels and limit it at very high levels, they can reduce noise and switch between different settings (programs) depending on the hearing situation [5]. Some hearing aids can “push” high-frequency signal components into lower frequency ranges if they are no longer accessible to the user there. In the case of bilateral hearing loss, a bilateral fitting should also be performed, if possible, to prevent deprivation of the unprovided ear and to improve speech understanding in noise. Conventional hearing aids improve hearing and speech understanding, but unfortunately cannot normalize it in most cases for various physiological reasons [6].
Cochlear Implants
If the hearing loss above 1 kHz is approximately 80 dB or above, then the hearing impairment is so severe that conventional hearing aids are of limited use. For these hearing disorders, cochlear implants (CI) are used in both adults and children from about the first year of life [7]. Cochlear implants replace the physiological function of the inner ear, i.e., the conversion of sound into action potentials of the vestibulocochlear nerve. Figures 2E and F show a current CI system. It consists of two parts. The sound is picked up by the microphone in the external speech processor (Fig. 2E), processed and sent transcutaneously via a radio link to the implant (Fig. 2F) located retroauricularly under the skin. Short electrical impulses are presented along the cochlea via today’s usually 12-22 electrodes according to the incoming acoustic signal, leading to auditory perception. Thus, the systems work even with complete deafness. Similar to hearing aids, cochlear implants today do not allow normal hearing, but the vast majority of adult users can use them to make phone calls, and children regularly learn language, including their local dialect, the same way as their normal-hearing peers. The shorter the duration of deafness before implantation, the better the chances of success in children and adults. Cochlear implants have already been called – and rightly so – “the most successful devices at the machine-brain interface” [8]. Today, around half a million people worldwide are already fitted with a cochlear implant.
Conclusion
Hearing disorders are particularly common in old age, but they also occur in children and are nowadays detected and treated at an early stage. Presbycusis particularly limits speech understanding in background noise and can lead to social withdrawal. Hearing aids are the treatment of choice for many mild to severe hearing losses, and for very severe hearing losses, cochlear implants can restore hearing in children and in adults.
Take-Home Messages
- Approximately 30% of people over the age of 65 suffer from significant and bilateral hearing loss. At birth, one in about 1000 children is affected.
- Conventional hearing aids in various designs are the most common type of appliance therapy. They can improve hearing and speech understanding in children and adults, but usually do not normalize it.
- In cases of very pronounced hearing loss or even complete deafness, the function of the inner ear can be taken over by a cochlear implant system in both children and adults, allowing hearing impressions to be restored and usually allowing open speech understanding.
Literature:
- Roth TN, Hanebuth D, Probst R: Prevalence of age-related hearing loss in Europe: a review. Eur Arch Otorhinolaryngol 2011; 268: 1101-1107.
- Bisgaard N, Ruf S: Findings From EuroTrak Surveys From 2009 to 2015: Hearing Loss Prevalence, Hearing Aid Adoption, and Benefits of Hearing Aid Use. Am J Audiol 2017; 26(3S): 451-461.
- Metzger D, Pezier TF, Veraguth D: Evaluation of universal newborn hearing screening in Switzerland 2012 and follow-up data for Zurich. Swiss Med Wkly 2013; 143: w13905.
- International Organization for Standardization: ISO Standard 7029: 2017.
- Hoppe U, Hesse G: Hearing aids: indications, technology, adaptation, and quality control. GMS Curr Top Otorhinolaryngol Head Neck Surg 2017; 16: Doc08.
- Lesica NA: Why do hearing aids fail to restore normal auditory perception? Trends Neurosci 2018 Feb 12; pii: S0166-2236(18)30032-8.
- Lenarz T: Cochlear implant – state of the art. GMS Curr Top Otorhinolaryngol Head Neck Surg 2018; 16: Doc04.
- Géléoc GS, Holt JR: Sound strategies for hearing restoration. Science 2014; 344: 1241062.
HAUSARZT PRAXIS 2018; 13(5): 29-31









