
There is still no specific treatment for pertussis or mononucleosis, so vaccination is highly recommended. Pertussis carries life-threatening complication risks, particularly in infants, and glandular fever can lead to Guillain-Barré syndrome in adolescents. Dr. med. Thomas Fischbach gave a practical overview of the most important childhood diseases and summarized the respective treatment measures, whereby the latter are usually only symptomatic in nature. Families should also consider follow-up pertussis vaccinations, as unvaccinated adults can infect young children.
The most common illnesses in childhood include banal respiratory infections, diarrheal diseases and conjunctivitis [1]. Measles, mumps, rubella (box) and hepatitis have become rarer nowadays thanks to standard vaccinations, but other vaccine-preventable diseases such as pertussis and glandular fever are still relatively common, according to Dr. Thomas Fischbach, a paediatrician in Solingen (Germany). Cases of HIV/AIDS, meningococcal infections and tropical infections are very rare. While many infections are self-limiting, others pose serious risks of complications.
Not every cold is dangerous
Banal respiratory tract infections are usually caused by viruses; bacterial infections are rather rare. It is well known that there are seasonal clusters in the winter months and the classic symptoms are a cold, cough and occasionally a fever. “Complications are usually caused by bacterial superinfections,” says Dr. Fischbach [1]. These include otitis media, sinusitis and pneumonia. Certain pathogens often cause spastic / obstructive bronchitis. The paediatrician reported that rhinoviruses, for example, lead to severe courses; he was aware of cases that went as far as hospitalization/requiring oxygen. Viral infections are treated symptomatically and medication should be used with caution. It is important to drink plenty of fluids and breathe fresh, smoke-free air. Decongestant nasal drops are important if a small child cannot breathe, especially babies (nasal breathers). Cough syrup can be useful for a child with an unproductive cough that causes sleep disturbances. In general, however, an increased incidence of respiratory tract infections in children is normal and antibiotics are rarely necessary. From the speaker’s point of view, it is problematic that since the corona pandemic, children have been sent home at the slightest sign of flu-like symptoms, which could conflict with adults’ professional activities [1].
| Pertussis can lead to severe apnea The most common pathogen causing whooping cough is Bordetella pertussis; B. parapertussis or B. homesii are less common. Mostly 2-6 year old children are affected. “It is a classic droplet infection that occurs all year round, more frequently in autumn and winter,” explained Dr. Fischbach [1]. The problem is that only around half of adults have sufficient vaccination protection and can infect children. The incubation period is variable 9-20 days, sometimes 9-10 days, whereby the infectiousness is particularly high in the first stage. The clinical presentation is divided into the catarrhal stage (1-2 weeks), the convulsive stage (4-6 weeks) and the decrementi stage (6-10 weeks), which is characterized by classic coughing fits. In children, the cough is accompanied by a rattling sound, while adults have a normal, persistent chesty cough. Possible complications of whooping cough include pneumonia, encephalopathies, seizures and respiratory distress. “Apnea in young infants is particularly feared,” the speaker emphasized [1]. Pertussis is a systemic infection that can disable the respiratory center. According to the speaker, this can lead to death in infants and appeals to the importance of vaccination. Unvaccinated parents should be re-vaccinated if necessary. If antibiotics are administered for whooping cough (first choice: macrolides), the main aim is to prevent the spread of the disease; it does not change the course of the disease very much [2,4]. |
Covid-19: antiviral for at-risk children?
Covid-19 is a SARS-CoV-2 droplet infection, in only 1% of cases the transmission route is a smear infection [1]. The incubation period is 3-4 days. Typical symptoms sometimes include high fever, severe headaches and aching limbs and occasionally shortness of breath/dyspnoea or gastrointestinal complaints. As we now know, Covid-19 infections in children tended to be mild and hospitalizations were rare. In contrast to RSV infections, this also applies to children at risk. The antiviral Paxlovid® is also effective and safe in children if taken within the first 5 days after the onset of symptoms [1]. Dr. Fischbach pointed out that Long-Covid is an issue that affects not only adults, but also adolescents, as he knows from his own everyday practice. “One girl is still in a wheelchair and has developed severe seronegative myasthenia gravis,” reported the speaker [1]. Initially, the Long Covid discussion in pediatrics was perhaps not taken seriously enough.
Respiratory syncytial virus (RSV): Vaccination for pregnant mothers?
RSV is a droplet infection with the highest incidence from November to April. In infants and small children – especially premature babies – this infection is dangerous and should be taken seriously. The incubation period is relatively short at 2-8 days. The symptoms range from simple respiratory diseases to severe respiratory diseases requiring ventilation. Typical symptoms are malaise, coughing, dyspnea, difficulty drinking and a poor general condition. Otitis media is a common complication, especially in children under 3 years of age [2]. Treatment is usually only symptomatic and it is important to ensure sufficient fluid intake. Immunization is possible for children at risk, for example premature babies or those with congenital heart disease. In addition to palivizumab (Synagis®) for passive immunization against RSV infections, the vaccine nirsevimab is also available in some countries [3,7]. The latter has the advantage that it only needs to be given once per season. There is also a vaccination for mothers in the 22-24th week of pregnancy. week of pregnancy, which leads to protection lasting up to 6 months in children [1].
Pfeiffer’s glandular fever: often inapparent in small children
Mononucleosis infectiosa is a classic smear infection and is sometimes also referred to as “kissing disease” or “student fever”. The incubation period can be up to 50 days. Classic symptoms are a cold, cough, watery eyes, sore throat and often a high temperature. The typical grayish-whitish coatings on the tonsils are a good distinguishing feature from streptococcal angina (purulent-yellowish coatings). The full manifestation of symptoms most frequently occurs in adolescence; in young children, the disease is usually inconspicuous, as can be concluded from EBV antibody detections as incidental findings. The spectrum of possible complications ranges from fatigue and Guillain-Barré syndrome to splenic rupture, Burkitt’s lymphoma and nasopharyngeal carcinoma are also possible. Treatment (e.g. fever reduction, high fluid intake) is given as required and is symptomatic in nature [4]. Fatigue, which can last for months, is very common.
Diarrheal diseases: Risk of complications due to exsiccosis
Diarrheal diseases are usually viral in origin and start suddenly with sometimes violent vomiting, which can sometimes lead to a stressful situation for children. Noroviruses and rotaviruses are the most common pathogens and can occur at any time of year; other bacteria such as salmonella, campylobacter or E. coli are less common. Rotaviruses are still common, even though they can be vaccinated against. In terms of the transmission route, these are classic smear infections; spread by droplet infection is rather rare. Typical clinical manifestations include diarrhea and vomiting, acute gastroenteritis, nausea and headaches. The state of health is often severely impaired. “The greatest danger in pediatrics is exsiccosis,” says Dr. Fischbach, adding: “This is not trivial” [1]. Dehydration can affect the eyes, lips and skin. Treatment is symptomatic and it is important to drink sufficient fluids (especially tea or water). Electrolyte solution is sometimes a little difficult with children, it may help if you enrich it with dextrose. Medication is usually not necessary. “The main thing is that they drink tea or water,” summarizes the speaker [1]. If antiemetics are administered for severe vomiting, it is important that the dosage is not higher than recommended on the package leaflet. Once the condition has improved and the diarrhea has stopped, the child can go back to daycare, kindergarten or school [2].
Conjunctivitis: Infection or foreign body exposure?
Most conjunctivitis is viral in origin, bacterial causes of infection are less common. Smear infection is the more common route of transmission; droplet infections are less common. The incidence is independent of age and season, the incubation period is 5-12 days. Typical symptoms are a reddened conjunctiva, watery eyes, sticky eyelids and secretions. Viral conjunctivitis is treated symptomatically with eye drops; if the cause of the infection is bacterial, antibiotics may be useful. Both eyes should always be examined and treated. If there is no reason to suspect a foreign body, the cornea should be inspected more closely. Rarely, corneal inflammation can develop as a complication. “The unilateral red eye is suspicious of a foreign body until it is refuted,” explained Dr. Fischbach [1]. Foreign bodies also include irritant gases. It should be borne in mind that conjunctivitis caused by herpes viruses usually starts on one side [2].
Aphthous stomatitis and hand-mouth-foot disease
Aphthous stomatitis, also known as oral thrush, is a droplet or smear infection caused by herpes simplex type 1 (HSV-1). Children are often in the 1st-4th grade. The incubation period is 1-26 days. In addition to painful aphthae in the area of the oral mucosa and associated swallowing difficulties, fever may also occur. In older children, only the throat and tonsillitis are often affected. Here too, treatment is symptomatic, pain-relieving mouth ointments are recommended and soft, cool food is best tolerated. Possible complications are exsiccosis and bacterial superinfections. [4]
Hand-foot-and-mouth disease (HFMD) is a viral infection caused by various Coxsackieviruses (primarily Coxsackievirus A) that occurs predominantly in young children (<10 years old). The occurrence of this infection is not seasonal and the incubation period is short. Droplet infection and smear infection are possible transmission routes, but you can also become infected in bathing water. The infection is highly contagious during the first week, especially in the case of ulcerating blisters. Possible symptoms include an itchy skin rash as well as ulcers on the tongue, gums or oral mucosa. In addition, affected children often suffer from a sore throat, reduced appetite and fever. The ulcerating blisters and pustules occur mainly on the hands, soles of the feet and trunk. “You can only treat symptoms,” says the speaker [1]. First and foremost, ointments against pain should be mentioned. It is very important that affected children drink enough. Complications are rare, the speaker has not had a case in 30 years of practice [1].
| Scarlet fever: complications can be serious The pathogens are group A streptococci, usually a droplet infection, contaminated food or contaminated water are rather rare. It occurs regardless of the season, usually in infants, but in rare cases adults can also become infected. There is a risk of infection for up to 3 weeks. In addition to fever, abdominal pain and vomiting, a skin rash in the cheek area or an exanthema, which typically begins inguinal or axillary and spreads, and the so-called “raspberry tongue” are typical. “If you don’t do anything, the skin on your hands or feet will eventually peel,” says Dr. Fischbach [1]. Penicillin is classically recommended for treatment, but cephalosporins or amoxicillin can be used. Acute rheumatic fever or glomerulonephritis can develop as complications. However, sepsis and peritonsillar abscesses are also possible. “This year we had a 6-year-old child who almost died from streptococcal sepsis,” reported the speaker [1]. Peritonsillar abscesses are relatively common complications in adults. A child affected by scarlet fever can return to nursery/kindergarten after 1-2 days with antibiotics; if you do not treat with antibiotics, you have to wait 3 weeks [1,2]. |
Chickenpox and rubella
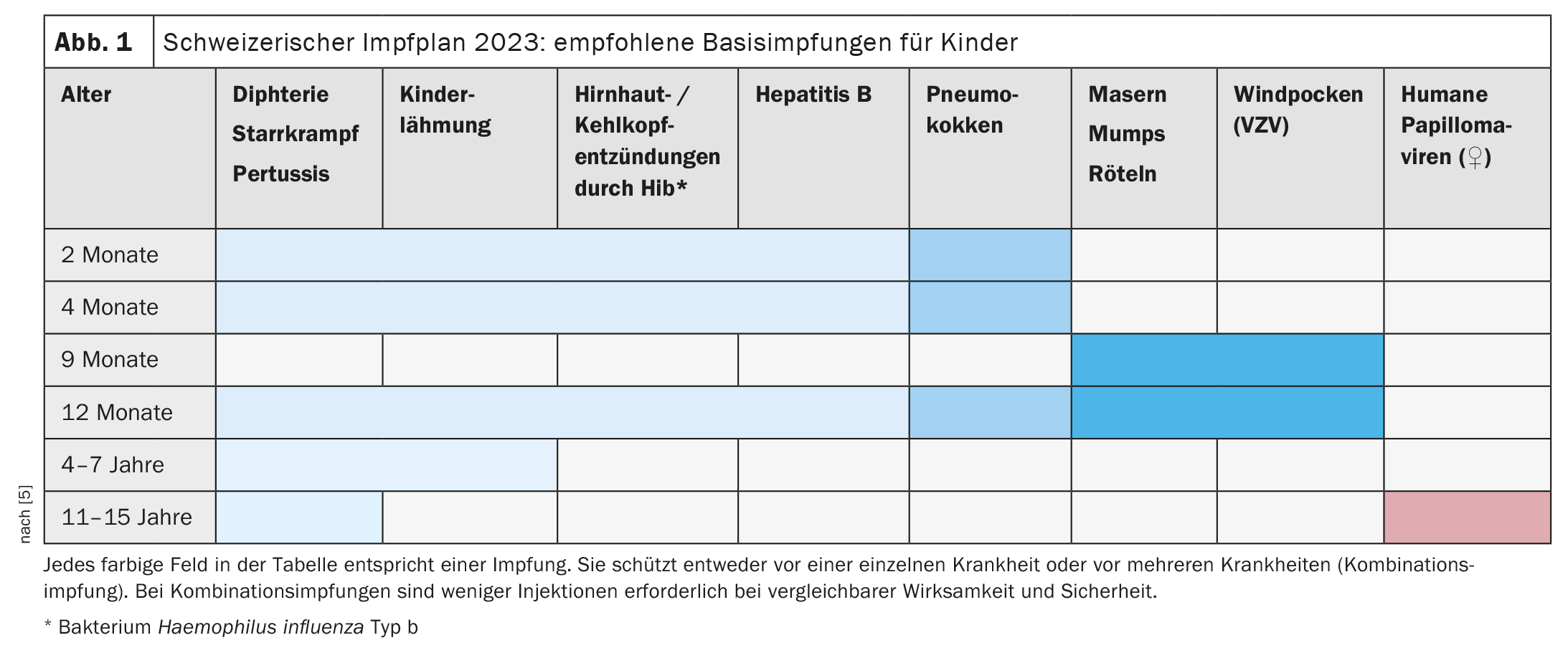
Chickenpox is caused by the varicella zoster virus (VZV) and is a classic droplet infection. The occurrence is independent of season and age. The incubation period is 14-21 days, and there is a risk of infection 2 days before the first blisters appear. The appearance is dominated by blisters, crusts and itching. A fever may occur. Fasciitis and cerebellar ataxia are known to be possible complications. Therapy is carried out syptomatically, primarily by means of antipruritic shaking lotion. 5 days after the appearance of fresh blisters, an affected child can return to nursery/kindergarten. In Switzerland, the VZV vaccination has been one of the basic vaccinations for children since 2023 [5]. If possible, a combined quadrivalent vaccine (measles, mumps, rubella, varicella) should be used. Adults can also be vaccinated against VZV.
Ringworm is also known as erythema infectiosum and is transmitted by the parvovirus B19 (droplet or smear infection). Infectiousness only exists before the rash appears. The incubation period ranges from 6-17 days. A garland-like rash is typical, as well as headaches and aching limbs, fever and a feeling of cold. Joint inflammation often occurs in adults. A complication that may occur in pregnant women with the disease is anemia in the child. Ringworm is also treated symptomatically [2].
Measles, mumps and rubella
The measles viruses spread via droplet infection. Measles is not simply a harmless childhood disease. The incubation period is 8-12 days, the preliminary stage is flu-like, from the 5th day of incubation until five days after the onset of the rash there is infectiousness. In addition to a severe rash and high fever, affected children may suffer from a cough and their general condition is often considerably impaired. Middle ear and lung inflammation can develop as a complication, but croup or encephalitis are also possible. As treatment measures, the speaker recommends bed rest, a darkened room and fever reduction [1]. He considers the measles-mumps-rubella vaccination to be very important.
The mumps virus is exclusively human pathogenic and also spreads as a droplet infection. The incubation period ranges from 14 to 24 days, infectiousness exists 7 days before to 9 days after the swelling appears. The swollen parotid glands and other salivary glands are often accompanied by a slight fever. Meningitis and orchitis (in boys) are known complications. The diagnosis is made clinically and by measuring alpha-amylase in the urine. Lymphadenopathy and sialadenitis must be ruled out in the differential diagnosis.
Rubella is caused by the rubella virus and should not be confused with ringworm. Like measles and mumps, rubella is also a droplet infection; the incubation period is 14-23 days, infectiousness is 6 days before to 7 days after the rash. In addition to a rash and swelling of the lymph nodes in the neck area, those affected often suffer from a slight impairment of well-being. Rare complications are encephalitis and arthritis (in adolescents and adults). Disease in unimmunized pregnant women can lead to embryopathy. Treatment is symptomatic. This is also a classic vaccine-preventable disease. In Switzerland, the vaccination coverage rate in 2022 was 94% (measles) and 93% (mumps and rubella) for 2-year-olds and 96% for 16-year-olds [6].
Literature:
- “What the family doctor should know about childhood diseases”, Dr. med. T. Fischbach, General Medicine Refresher Cologne, 17-20.01.2024.
- RKI-Ratgeber (online), www.rki.de/ratgeber,(last accessed 29.01.2024)
- Swissmedic: Medicinal product information, www.swissmedicinfo.ch,(last accessed 29.01.2024)
- Pediatricians on the net: Diseases A-Z (online): www.kinderarzte-im-netz.de/krankheiten,(last accessed 29.01.2024)
- “Vaccinations for infants and children”, www.bag.admin.ch/bag/de/home/gesund-leben/gesundheitsfoerderung-und-praevention/impfungen-prophylaxe/impfungen-fuer-saeuglinge-und-kinder.html,(last accessed 29.01.2024)
- Trageser J, et al: Evaluation of vaccination promotion and increasing vaccination readiness, final report, Federal Office of Public Health, 2023.
- Swissmedic: Medicinal product information, www.swissmedicinfo.ch,(last accessed 30.01.2024)
HAUSARZT PRAXIS 2024; 19(2): 38-40 (published on 20.2.24, ahead of print)









