
The hands reveal the true age – so they say. In fact, they usually show the most pronounced symptoms of so-called extrinsic skin aging, also called photoaging. Consistent sun protection is essential to prevent photodamage. If the hands already show signs of photo-aged skin, various therapies such as lasers, fillers or topicals are available. These can be used in isolation or in combination and show good results.
A distinction is made between intrinsic, i.e. natural skin aging, and extrinsic aging. Sun and artificial UV light (called photoaging), but also smoking, excessive alcohol consumption and malnutrition have an impact on the condition of the skin. The difference between intrinsic and extrinsic skin aging becomes particularly clear when the hands are placed on the lower abdomen. While abdominal skin and hand skin have the same age, they differ in the intensity of chronic sun exposure.
Solar radiation as a central factor
Naturally aged skin is usually soft and unblemished. Sun-exposed areas, on the other hand, show wrinkles, pigmented lesions such as freckles, lentigines and patchy hyperpigmentation, but also depigmentation (hypomelanosis guttata). A loss of tone and elasticity and a tendency to purpura and ecchymosis, due to skin fragility and weakness of blood vessels, are observed. Thus, light-damaged skin can be clearly identified histopathologically: It is characterized by epidermal atrophy, fragmented and thickened collagen fibers, and fragmented elastic fibers with cross-linking and calcification.
It is now generally agreed that the thickness of the stratum corneum does not change with age. What does change, however, is the dermo-epidermal junction and the so-called “cell turnover”. This explains the fragility and slowed healing of the skin with age [1]. More distinct differences are seen in the dermis, where about 20% of dermal thickness shrinks with age. Subcutaneous adipose tissue also reduces – especially on the face and on the backs of the hands and edges of the shins, while it tends to accumulate on the hips of women and the abdomen of men, respectively. Thus, the hand veins become more prominent on an aged hand.
A dry, flaky texture continues to be part of the appearance of older skin. On the one hand, this is due to the fact that a damaged barrier function can only be regenerated slowly, but on the other hand, it is also due to an increased transepidermal water loss (TEWL) [2]. These symptoms are particularly evident on the hands. The backs of the hands are so-called sun terraces, which tend to form neoplasms due to light damage (Fig. 1).

Prevention of photodamage: sun protection
It is undisputed that sunscreens protect against the development of actinic keratoses. But its cosmetic benefits have also been proven: A study with children showed that the use of SPF 30 resulted in 30-40% less freckle development. Accordingly, hand creams with sunscreen are recommended, but unfortunately the industry has so far only little adapted to this indication. Alternatively, textile sunscreen can be recommended – as practiced in ancient times or still by Asians today.
Retinoids inhibit collagenase synthesis and promote collagen production [3]. Studies have also shown the anti-oxidant effect of vitamins C and E combined with ferulic acid or the effect of green tea [4]. Such combinations find use in cosmetics.
Therapy options
Our therapies refer partly combined, partly isolated to the three main symptoms of light-aged hands: Spots, loss of volume, and changes in surface skin texture (roughness and dryness).
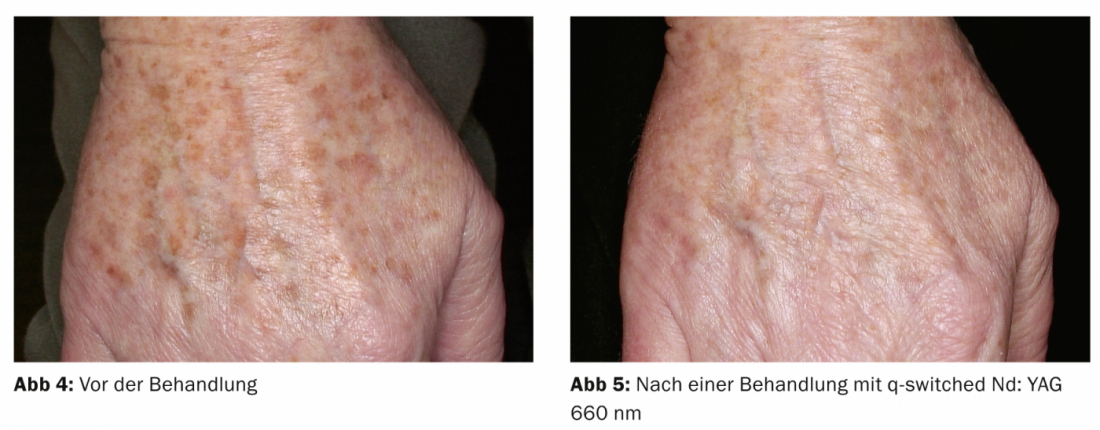
For spots – lentigines solares – q-switched laser is the first choice after careful exclusion of atypical lesions. The q-switched ruby laser (649 nm) and the q-switched NeoDym YAG laser (frequency doubled, 532 nm) are most commonly used (Fig. 2-3).

Some manufacturers now also offer the interesting wavelength 660 nm, which causes fewer vascular side effects (Fig. 4-5).
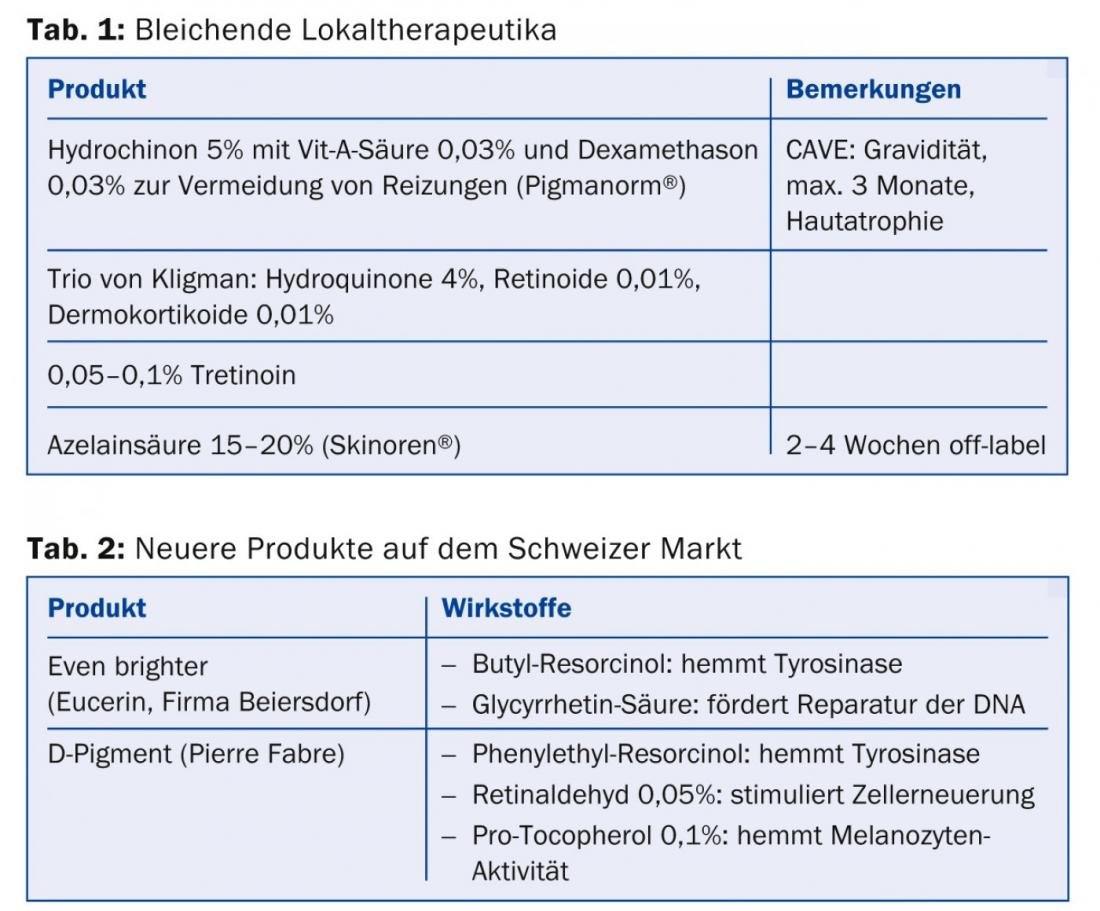
In contrast, the 2006 Pigmentary Disorders Academy consensus protocol recommended ablative cryotherapy for lentigines [5]. Alternatively, bleaching creams and solutions, as listed in Tables 1 and 2, can be used. With deeper pigment, however, only few effects are to be expected here. Better penetration can be expected when bleaching products are used in conjunction with exfoliation procedures.
To prevent volume loss, hyaluronic acid, calcium hydroxylapatite and autologous fat are suitable filler materials. However, due to the thinner skin on the back of the hand, these therapies should only be practiced by experienced practitioners. More strongly cross-linked hyaluronic acid, for example, can lead to undesirable “puffy hands” because of its strong water-binding capacity, and very unpleasant granuloma formation has been described in some cases with calcium hydroxyapatite.
If the volume loss is not yet so pronounced, mesotherapy can start directly in the dermis. By increasing the reduced hyaluronic acid concentration, the formation of collagen and elastin is stimulated. In addition, the method leads to an improvement in hydration. However, a real film effect should not be expected.
Other technical possibilities
Fractionated lasers (CO2 and erbium) and fractionated radiofrequency, which is particularly well tolerated in the hand area, also have positive effects on the dermis and epidermis (Figs. 6-7).

The surface structure is improved, the skin appears less rough and dry. Both non-ablative and ablative systems are aimed at so-called “rejuvenation”, which is a controlled form of wound healing with the goal of a more youthful appearance of the skin. Since the hand area cannot be treated as aggressively, expect at least three sessions.
Literature:
- El-Domyati M, et al: Intrinsic aging vs. photoaging: a comparative histopathological, immunohistochemical, and utrastructural study of skin. Exp Dermatol 2002; 11(5): 398-405.
- Baumann L: Skin aging and its treatment, J Pathol 2007; 211: 241-251.
- Kang S, Fischer GJ, Voorhees JJ: Photoaging and topical tretinoin; Arch Dermat 1997, 133: 1280-1284.
- Lin FH, et al: Ferulic acid stabilizes a solution of vitamins C and E and doubles is photoprotection of skin. J invest Dermatol 2005; 125 (4): 826-832.
- Ortonne JP, et al: Treatment of solar lentigines. J Am Acad Dermatol 2006; 54(5S2): 262-271.
DERMATOLOGIE PRAXIS 2014; 24(4): 22-24









