Hyperproliferation of the three cell series in the bone marrow causes erythrocytosis, thrombocytosis, and leukocytosis in polycythaemia vera. The result is, among other things, a significant increase in hematocrit levels and thus also in the risk of thromboembolic events. With acetylsalicylic acid (ASA), phlebotomies, and cytoreductive agents, several options are available to prevent thrombosis. But which is indicated when?
Polycythaemia vera (PV) is a very rare, chronic myeloproliferative neoplasia and is characterized by increased hematopoiesis. The majority of PV patients have a mutation in the JAK2 tyrosine kinase gene [1]. It results in increased cell proliferation as well as increased production of proinflammatory cytokines. The overproduction of erythrocytes and consequently increased hematocrit levels increase blood viscosity. In this way, the occurrence of thromboembolism is favored: 45% of all deaths in PV are due to thromboembolic complications [2].
Although the symptoms are varied, they are often very non-specific. Therefore, the diagnosis is often made only by chance. Possible symptoms include headache, visual disturbances, fatigue and pruritus, as well as bone pain and pain in the upper abdomen. These are often caused by splenomegaly typical of PV [1,2]. The increased blood cell mass can cause circulatory disturbances that can lead to severe venous and arterial thrombosis such as pulmonary embolism, apoplexy, or myocardial infarction. Therefore, early diagnosis and effective therapy are indicated (Table 1) [3].

Risk-adapted treatment
Because prevention of thromboembolism is paramount, phlebotomy is often considered the treatment of choice. Thus, the hematocrit (Hct) can be lowered to below 45% and the hyperviscosity of the blood can be reduced. Studies have shown that setting Hct below 45% can reduce the rate of cardiovascular death in PV to one quarter [4]. However, a phlebotomy is very tiring. Therefore, in low-risk patients, additional treatment with low-dose acetylsalicylic acid (ASA) is recommended. A low risk can be assumed in younger patients <60 years who have not had thrombosis before.
Cytoreductive therapy in high-risk patients.
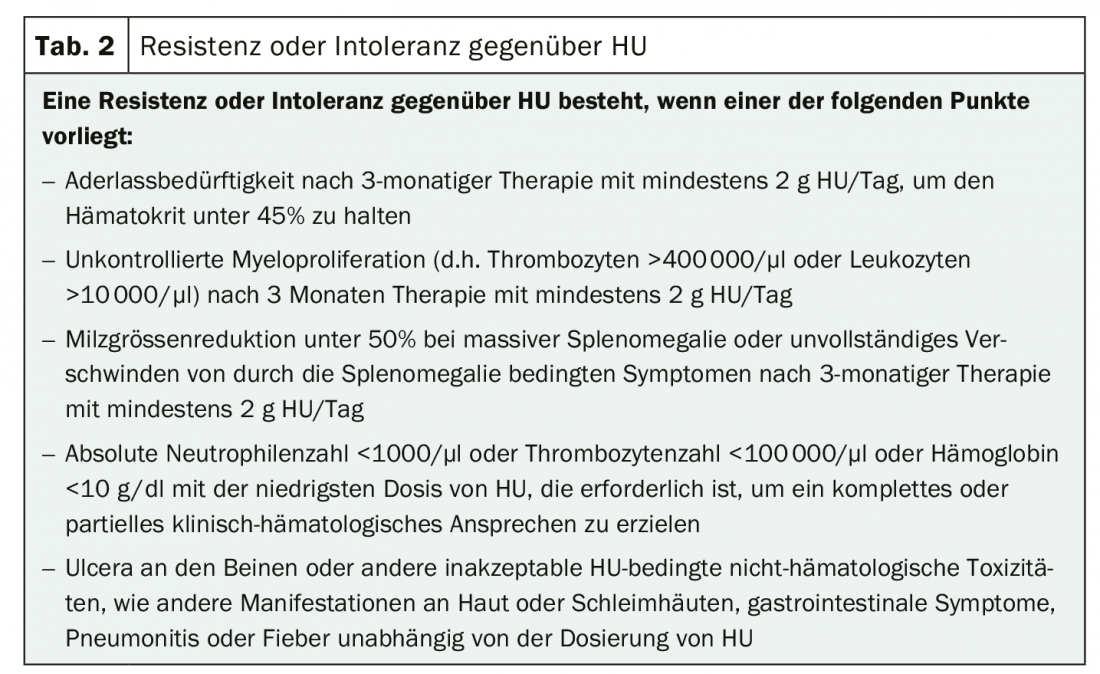
However, the majority of PV patients are at high risk. In them, initiation of cytoreductive therapy is indicated. Hydroxyurea (HU) or interferon alpha (INF) are recommended for primary treatment [5]. However, HU in particular is not suitable for all patients and can cause severe side effects (Table 2) [6]. Therefore, INF is more commonly used in younger patients of childbearing potential. If first-line therapy is not tolerated or clinical symptoms do not resolve sufficiently, treatment should be switched. The JAK2 inhibitor ruxolitinib has been shown in trials to control increased myeloproliferation while being well tolerated [1]. Many PV-associated symptoms, such as fatigue and pruritus, also regressed. In addition, the effect occurred very quickly in most patients, within the first four weeks. Busulfan can be used as an alternative therapy in patients of advanced age. However, the leukemogenic potential of this substance is always under discussion, which is why it should only be used with restraint. Anagrelide may be considered as a combination partner to, for example, HU or INF. This is aimed exclusively at reducing platelet production and can act as a supplement if satisfactory results are not achieved with the other substances alone.
Literature:
- www.onkopedia.com/de/onkopedia/guidelines/polycythaemia-vera-pv/@@guideline/html/index.html (last call on 10.05.2020)
- Vannucchi AM, et al: N Engl J Med 2015; 372: 426-35.
- Stein BL, Moliterno AR, Tiu RV: Polycythemia vera disease burden: contributing factors, impact on quality of life, andemerging treatment options. Ann Hematol 2014; 93: 1965-1976.
- Marchioli R, Finazzi G, Specchia G, et al: Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med 2013; 368: 22-33.
- Barbui T, Tefferi A, Vannucchi AM, et al: Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European Leukemia Net. Leukemia 2018; 32: 1057-1069.
- Barosi G, Birgegard G, Finazzi G, et al: A unified definition of clinical resistance and intolerance to hydroxycarbamide in polycythaemia vera and primary myelofibrosis: results of a European LeukemiaNet (ELN) consensus process. Br J Haematol 2010; 148: 961-963.
InFo ONCOLOGY & HEMATOLOGY 2020; 8(3): 31.









