
The “main players” in the filler market are all recommendable. However, there are differences in lifting capacity, swelling potential, durability and rheological application. The choice of products is made individually.
Welcome to a new series in the Aesthetic Dermatology Continuing Education Series! After the topics “Botulinum” (DERMATOLOGIE PRAXIS 01/15, 02/16, 04/17 and 06/17) and “Peeling”(05/15 and 06/15) have been completed, we now turn to the topic “Filler”. As usual, we will also divide this large subfield of aesthetic dermatology into several chapters so that it can be conveyed to you as the reader in as much detail as possible on the one hand, and on the other hand so that the reading does not take up too much time. We are all busy and are happy to be informed briefly and yet scientifically accurate after the day’s work is done.
We distinguish degradable from non-degradable filling materials. With the non-degradable materials, disfiguring reactive knot formation occurred in some cases, which is why these products were withdrawn from the market years ago. Since reactive nodules can still occur today – decades after injection has taken place – it is nevertheless important to be aware of these products. But now one after the other…
Non-degradable filling materials
It is understandable that the desire on the part of patients for permanent fillers has been implemented by the industry. The fact that treatment with fillers has to be repeated due to their degradation is complained about by patients practically at every preliminary medical consultation (“But you have to repeat that all the time? How long does the effect last?”). Non-absorbable filling materials consisting of polyacrylamide (Aquamid®), polymethyl methacrylate and collagen (Artecoll®, Artefill®) or hydroxyethyl methacrylate (Dermalive®) really boomed about 20 years ago. Finally, similar to surgery, permanent results could be promised. The unsightly complications with sometimes grotesque granuloma formations after silicone-containing implants, as was common especially after gender operations in the late 60s and early 70s of the last century, were forgotten. However, it was not long before the first reports of unsightly knot formation were also scientifically reported with these non-degradable filling materials, which is why they were eventually withdrawn from the market again relatively quickly. Even today – years after initial treatment – reactivation of these substances occurs after reinjection of hyaluronic acid-containing and thus degradable fillers. We then talk about so-called biofilms or reactive granulomas depending on the doctrine. The existence of biofilms is controversial: These are said to be infectious encapsulated systems that remain inert in the skin and are formed by the introduction of skin-specific bacteria after injection. After renewed treatment, these are activated and sometimes sterile purulent inflammatory granulomatous nodules form in the injection area, rarely also at sites remote from treatment. This reaction can occur – as mentioned – years after treatment with non-degradable filling materials after re-injection with harmless hyaluronic acid. Therefore, their knowledge is of eminent importance when treating patients with fillers. Therapy for this complication ranges from systemic antibiotic prescription to local steroid injections to surgical sanitation, depending on the severity of the granulomatous reaction.
Degradable filling materials
Hyaluronic acid preparations are particularly worthy of mention here. Other degradable preparations with clinical study data include calcium hydroxyapatite (Radiesse®) and polylactic acid (PLA), also known as polylactic acid (Sculptra®). Strictly speaking, the latter is not a filler but a dermal stimulator of collagen fibers. Due to the technical difficulty of applying polylactic acid (the powder-like substance must be dissolved and usually remains inhomogeneous), reactive nodule formation (different concentration amounts) very often occurs, which is why this filler can only be conditionally recommended for extremely experienced users. Calcium hydroxyapatite has a significantly higher lifting capacity compared to HA, which is why less material needs to be applied to achieve an esthetically correct result. Unlike HA with hyaluronidase, there is no dissolving enzyme for either polylactic acid or calcium hydroxyapatite, so any technically induced nodule formation or overtreatment cannot be corrected.
Naturally occurring hyaluronic acid and non-crosslinked fillers
Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan in the human body. Approximately 50% of the skin consists of hyaluronic acid as an extracellular matrix. Furthermore, it is the most important component of the synovial fluid and the vitreous humor of the eye. In the skin, HA as an intercellular substance is responsible for structure maintenance and volume and ensures the necessary hydration of the skin, this because of the incredible water binding capacity of HA (more than 1000 times the binding capacity of its own volume). For a 70 kg person, we find about 15 g of natural HA. The half-life of naturally occurring HA is very short, about 24 hours, and about one-third of the total amount is metabolized or absorbed within one day. renewed. With age, the formation and also the turnover of HA decrease drastically, among other things an important reason for the continuous aging with slackening of the tissue with the consecutive consequences of wrinkles, the increasingly thinner skin as well as the so-called “sagging”. The mechanism of action of native (i.e. non-cross-linked, naturally occurring) HA is the stimulation of fibroblasts via cell-to-cell communication (“biosignaling”), improvement of skin elasticity, turgor, and hydration of the dermis. These properties are exploited in the so-called skin boosters. However, the syrupy native HA has no lifting capacity, which is why HA in fillers is changed to a gel-like substance by means of crosslinking.
Chemical modification of hyaluronic acid for clinical use
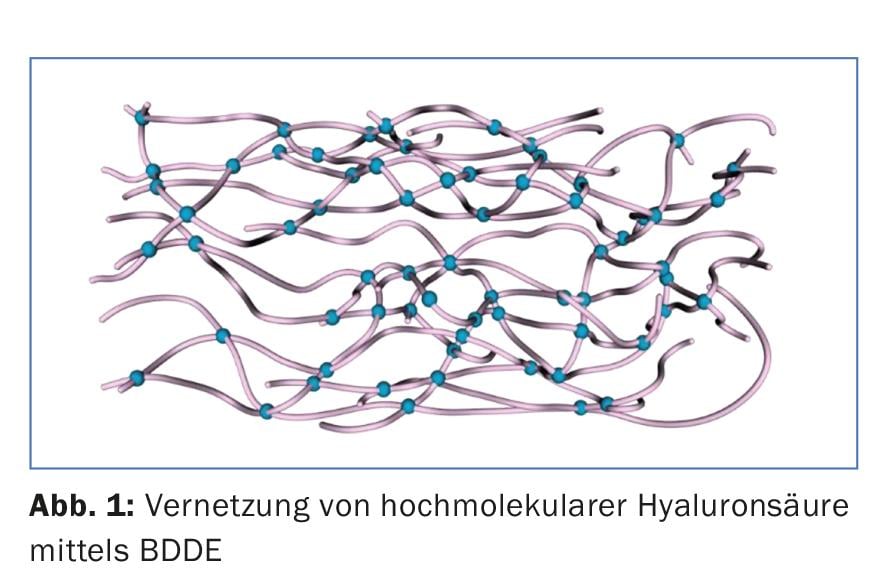
In order to achieve the mechanical properties, especially the volume effect of HA and to improve the durability due to the extremely short half-life, the commercially available HA are crosslinked and/or chemically modified. There are biphasic HA fillers (Restylane®) and monophasic (Juvéderm®, Belotero®, Teosyal® etc.). In the case of biphasic fillers, the so-called NASHA technique (“non-animal stabilized hyaluronic acid”) is used to cross-link particles of different sizes depending on the desired degree of viscosity, while in the case of monophasic fillers, synthetic cross-linking is carried out by means of BDDE (1,4-butanediol-diglycidyl ether). (Fig. 1). Because of the better rheology (flow property of a liquid), monophasic HA products are preferred nowadays. Their strength is achieved on the one hand by increasing the HA concentration and on the other hand by increased crosslinking by means of BDDE (so-called “crosslinking”). The higher the degree of crosslinking using BDDE or the higher the HA concentration of an HA gel, the firmer the network and the more viscous the gel becomes. The HA concentration of the various HA products is always indicated. Interestingly, it has been shown that the duration of action of HA products depends neither on particle size (biphasic fillers) nor on concentration (monophasic fillers), but solely on the number of crosslinkings. In order to improve the rheology and thus to reduce the squeezing pressure of the HA out of the syringe, the tendency nowadays is to obtain the viscosity not so much by increasing the HA concentration, but rather by increasing the crosslinking.
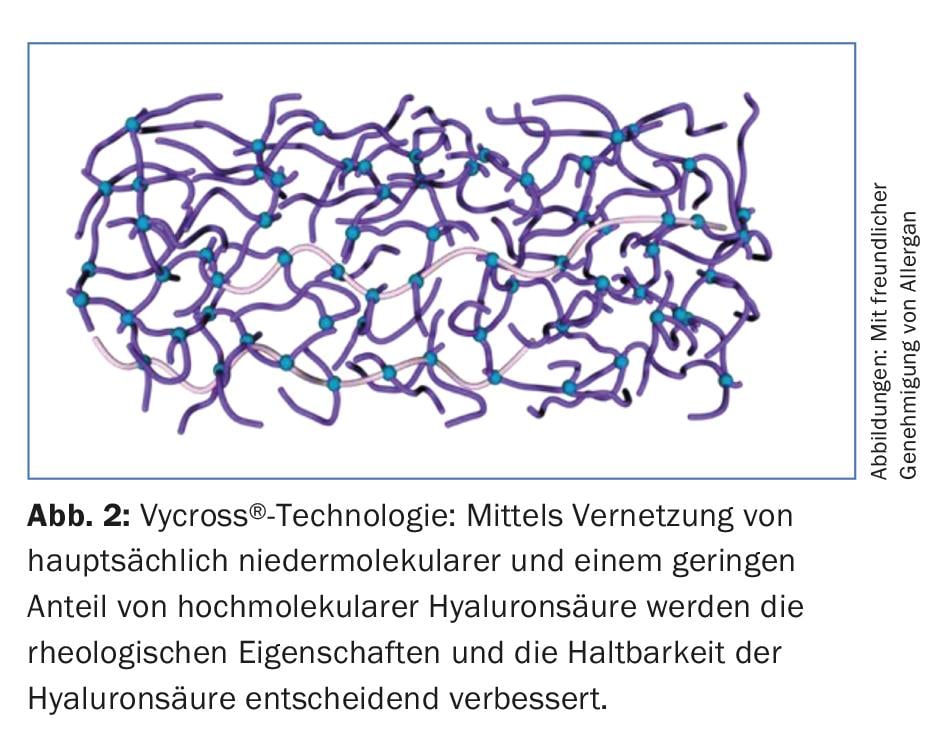
Vycross® technology is a further development of crosslinking. While conventional crosslinking involves exclusively crosslinking high-molecular HA using BDDE, the Vycross® technology crosslinks predominantly low-molecular HA with a small proportion of high-molecular HA (Fig. 2) . This results in several advantages that can be used in everyday clinical practice. First and foremost, the rheological properties improve, and the squeezing pressure from the syringe is noticeably reduced. In addition, the increased crosslinking results in greater degradation resistance and thus a longer duration of action on the one hand, and minimal swelling on the other hand due to lower water absorption as a result of lower HA concentration.
Clinical application of the different viscous HA gels
The strength or stability of an HA filler is indicated by the so-called “elastic modulus” G’ (pronounced: “Tschi praim”). The more viscous the gel (high G’), the greater its lifting capacity, and conversely the more liquid the gel (low G’), the less lifting capacity and the more malleable the HA. The G’ thus has a direct influence on the choice of an HA filler depending on the therapeutic need resp. Localization of the treatment. Products with a high G’ are used when a large lifting effect, i.e. actual volumization, is desired (e.g. augmentation of the midface, Os zygomaticum, or the nasolabial fold or temple area). Due to the high viscosity, a thicker needle (e.g. 25-23 G instead of the usual 27 G) must be used, which in turn has an influence on the injection technique itself. Products with a high G’ are usually applied sharply with the needle using the bolus principle (or the tower principle according to G. Sattler). The gel-like substance is injected perpendicular to the skin surface in a point-like manner (bolus) very deeply at the level of the bony structures in order to obtain a lifting effect that is as homogeneous as possible. The application system was refined by Maurizio de Maio with the so-called MD-Codes®. This is a subcutaneous injection technique in which the hyaluronic acid is not injected directly under the wrinkles, but deeply at anatomically crucial points. These areas are important for the reconstruction of the natural facial contour. By compensating for the loss of volume, the natural facial features are restored, making the face look fresher and younger. Hyaluronic acid products with a high G’ are thus used for deep augmentations when a high lifting capacity is desired (volumization). These products have the disadvantage of less malleability and entail greater swelling post interventionem. However, the shelf life is decisively extended compared to products with lower G’.
Products with a lower G’ are used for finer facial corrections on more superficial areas of the skin. They are less viscous, i.e. more liquid, and are therefore easier to shape and have a lower squeezing pressure. Examples of applications for these products are superficial wrinkles, sometimes in technically difficult to approach areas such as suborbital, or augmentation of lips. With the development of the flexible, relatively long blunt cannula, the injection technique for the superficially applied, less viscous hyaluronic acid products was decisively changed. The blunt cannula is used to apply the superficially injected fillers from a point in a fan-shaped manner (“windmill technique” according to Gerhard Sattler). Depending on the problem, it has proven useful to combine the deep injection technique with relatively solid gel-like products (high G’) with a second superficial pass with relatively liquid fillers (deep G’). In this case, we speak of the so-called “sandwich technique”. So, in summary, it’s no longer a case of “a filler is a filler.” For a harmonious aesthetic result without unsightly overcorrections, knowledge and correct application of the various fillers available on the market are crucial. Faulty results are very often due to ignorance of the various fillers and thus the incorrect use of the material.
Which filler do you take now?
As mentioned above, for deep volumization such as midface reconstruction, a viscous filler with higher concentration and greater cross-linking must be chosen, while for superficial fine wrinkle correction or in difficult areas such as suborbital or lips, a filler with lower viscosity is injected. The ideal filler demonstrates an excellent safety profile while being as long-lasting as possible. In terms of safety, a filler must be highly biocompatible. It should not have any hypersensitivity potential and should cause as little inflammation as possible after injection, resulting in swelling and later granuloma formation. The duration of effectiveness has already been mentioned. In addition, an ideal filler must remain stably in place and must neither clump nor migrate in response to gravity. Today’s fillers must also meet high standards in terms of practicality. The filler must have rheological properties that allow easy injection with the best possible deformability and light squeeze-out pressure. In terms of effectiveness, a high degree of lifting capacity (in the case of low volumetrics) or a high degree of of deformability (e.g. for reconstruction of the lips) is desired. In addition to its lifting capacity, an ideal filler also has other bioactive properties such as stimulation of collagen production.
In general, it can be stated that all products available on the European market are biocompatible and therefore safe. The “main players” in the filler market are all recommendable. There are differences in lifting capacity, swelling potential, durability and rheological application, with no “black sheep”. Certainly, a product must be chosen that is “FDA-approved” – it is recommended to choose a product with a proven study record. Even among experts with many years of experience in the use of fillers, there are always academic discussions about the best filler. Experience brings an individuality of product choice from practitioner to practitioner. The beginner is recommended to gain experience with products of the leading companies, and then create your own range of products.
What are skin boosters?
The technique of “skin boosting” has just recently experienced a renaissance. Already more than ten years ago, this technique was developed and subsequently fell more and more into oblivion. This is due to the questionable effectiveness of the products at that time, on the one hand, and on the other hand, due to the downtime (social time-out after treatment) caused by small bleedings, hematomas and long-lasting wheal formation as a result of delayed integration of the filler into the tissue. The effectiveness could now be significantly improved with the newly developed fillers, so that skin boosting can definitely be given its justification. The direct side effects (flea bite-like bleeding or hemorrhaging, temporary wheal formation) after injection remain, but the annoying mosquito bite-like wheals, which can last for weeks, no longer occur with modern products. The wheal formation is no longer visible after only a few hours post interventionem.
In skin boosting, tiny amounts of native HA are injected intradermally at intervals of about 0.5 cm. Due to the strong water binding capacity of HA, a velvety planar augmentation occurs over time in the area of the injected area. Due to the hydration of the skin, it is possible to speak of a long-lasting internal “face mask”. With repetitive use, age-related HA degradation can thus be elegantly counteracted. The skin becomes visibly finer, also smoother and acquires a youthful glow. The mechanical stimulation with the multiple injections stimulates the fibroblasts and results in increased collagen synthesis and thus, with multiple applications, visible tightening of the facial skin. With this technique, vertical lip wrinkles (“barcode lines” or “smoker lines”) and the so-called “sleeping lines” in the décolleté area can now finally be effectively addressed.
On the downside, native HA has a relatively short half-life and thus treatments (at least initially) have to be performed every six to twelve weeks. With Vycross®-developed products, a significantly longer shelf life of six months can be achieved, resulting in a decrease in the need for treatment without compromising effectiveness.
Take-Home Messages
- With the non-degradable filler materials, reactive nodules may still occur decades after the injection has been performed.
- Among the degradable filling materials, hyaluronic acid preparations are particularly noteworthy. Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan in the human body. For clinical use, it is chemically modified.
- The so-called “elastic modulus” G’ (strength or stability) has a direct influence on the choice of an HA filler – depending on the therapeutic need resp. Localization of the treatment. Products with high G’ are used when a large lifting effect is desired. Products with lower G’ are used for finer facial corrections on more superficial areas of the skin.
- The technique of “skin-boosting” (smallest amounts of native HA intradermally at a distance of about 0.5 cm) has just recently experienced a renaissance.
DERMATOLOGIE PRAXIS 2018; 28(5): 25-28









