
Hand eczema has far-reaching medical and socio-economic consequences. Rapid, efficient therapy and identification of trigger factors are necessary to prevent recurrences and chronic courses. The cornerstones of step therapy are baseline lipid-replenishing therapy, the use of topical corticosteroids and calcineurin inhibitors, UV irradiation, and, if response is inadequate, alitretinoin or immunosuppressants.
Hand eczema is very common [1], tends to be chronic [2], and significantly affects quality of life [3]. They not only affect the patients but also have far-reaching social and economic consequences [4]. Therefore, timely diagnosis, cause clarification and therapy initiation are of immense importance. A consensus paper summarizing the most important clinical aspects, diagnostic measures and a stepwise therapy was written by experts from the Dermatoallergology Working Group of the Swiss Society of Dermatology and Venereology (SGDV) [5].
Classification of eczema
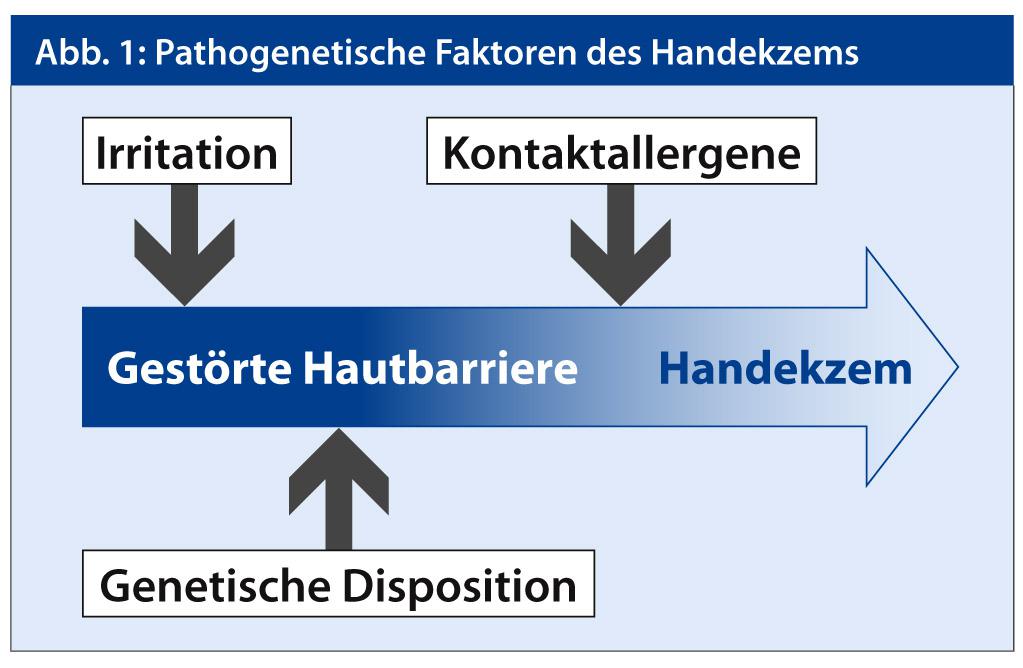
Hand eczema is classified according to its etiology and, if this is not possible, according to its morphology. The most common is irritant contact dermatitis. Numerous occupational hand eczema caused by wet work, prolonged wearing of rubber gloves, frequent and intensive washing, application of detergents fall under this heading. Irritant eczema is often a precursor to allergic contact dermatitis. Atopic hand eczema occurs in isolation or in association with other skin manifestations, allergic rhinitis, and/or bronchial asthma. Due to the genetically determined disturbance of the barrier function, the skin is particularly sensitive to external influences. In clinical practice, a combination of these eczema types is frequently encountered, for example, irritant contact dermatitis with predisposing atopic dermatitis onto which a contact allergy is grafted (Fig. 1).
Morphologically, dyshidrosiform, hyperkeratotic-rhagadiform and nummular eczema can be distinguished.
Severity
The severity of hand eczema is determined primarily by the extent and clinical signs, but also by the duration, the response to therapy, and the degree of suffering. Hand eczema that heals spontaneously, with avoidance of triggers, or in response to adequate therapy within three months is considered acute [6]. Hand eczema persisting for more than three months or recurring several times (>2 per year) is defined as chronic [6]. Various scores are available to measure severity, which include the extent and intensity of disease signs such as erythema, infiltration, vesicles, fissures/rhagades, scaling, and edema, for example “Hand ECzema Severity Index” (HECSI) and “Osnabrück Hand eczema Severity Index” (OHSI) [7, 8]. Photo boards with examples of mild, moderate, and severe hand eczema have also proven useful for clinical trials and everyday practice [9].
Impact on quality-of-life
Hand eczema has a significant impact on patients’ personal, social and professional lives. They significantly affect the quality of life of those affected [3]. The limitations are comparable to those in psoriasis or asthma patients [3]. In patients with occupational hand eczema, impairment of quality of life correlates with clinical severity [10]. Severe hand eczema was significantly more often associated with symptoms of anxiety and depression [10].
Late treatment increases risk of chronicity
A study from Denmark highlights that the prognosis of hand eczema worsens with each month of delayed medical treatment [2]. The more time that passes before hand eczema is diagnosed, the higher the risk of a chronic course [11].
Diagnostics
The diagnosis of hand eczema can be made clinically in most cases, taking into account the differential diagnoses. If allergic contact dermatitis is suspected, an epicutaneous test is indicated (Fig. 2). Based on a detailed medical history, potential allergens from the patient’s professional and private environment should be tested. It is important to determine the relevance of contact sensitization to hand eczema in the case of positive test reactions.

Step therapy
For the management of hand eczema, the basic insights into pathogenesis are crucial: restoration of the skin barrier and reduction of inflammation are needed. For practical reasons, a stepwise approach to treatment is recommended (Fig. 3) [5]. Basic lipid-replenishing therapy should be consistently applied alone or in combination with other anti-inflammatory measures. In addition, gentle cleansing and skin protection are recommended according to the individual external skin stress. External trigger factors such as irritants, moisture and humidity or contact allergens should be avoided.

Topical corticosteroids (at least class 2) are primarily used for therapy. They are particularly appropriate for short-term therapy when class 4 steroids are prescribed. Interval treatment may be used for long-term therapy. In addition to inhibiting inflammation, topical calcineurin inhibitors lead to restoration of the skin barrier [12]. Furthermore, UV therapy with UVB or PUVA may be considered.
If these measures are not sufficient, systemic therapy is indicated. Alitretinoin, which is approved for the treatment of severe chronic hand eczema, is a suitable option for this purpose. Alitretinoin is usually dosed at 30 mg per day and administered over a period of three to six months. The risk and side effect profile of retinoids must be considered. Acitretin, a retinoid approved for the treatment of keratinization disorders, can also be administered. If there is an inadequate response or contraindications to retinoids, other immunosuppressive drugs may be helpful. Ciclosporin was studied in patients with chronic hand eczema and showed a good effect. Data on the efficacy of azathioprine, methotrexate, and TNF-alpha blockers are available from casuistry and case series [5]. Systemic corticosteroids should be used only for acute exacerbations of hand eczema, often showing a rapid effect, but are not suitable for longer-term treatment.
Conclusion
The effects of hand eczema are far-reaching. Rapid diagnosis and initiation of therapy are prerequisites for rapid and complete healing of hand eczema. Long-standing and severe hand eczema tends to become chronic. Trigger factors such as irritants and contact allergens should be identified and avoided. Treatment should be given in stages and includes systemic therapy. Hand eczema patients must be trained extensively, individually, and repeatedly, as appropriate, in the use of skin care and protective measures to prevent recurrences and chronic courses.
Literature:
- Meding B, Järvholm B: Hand eczema in Swedish adults – changes in prevalence between 1983 and 1996. J Invest Dermatol 2002; 118: 719-723.
- Hald M, Agner T, Blands J, Johansen JD; Danish Contact Dermatitis Group: Delay in medical attention to hand eczema: a follow-up study. Br J Dermatol 2009; 161: 1294-1300.
- Moberg C, Alderling M, Meding B: Hand eczema and quality of life: a population-based study. Br J Dermatol 2009; 161: 397-403.
- Augustin M, Kuessner D, Purwins S, Hieke K, Posthumus J, Diepgen TL: Cost-of-illness of patients with chronic hand eczema in routine care: results from a multicentre study in Germany. Br J Dermatol 2011; 165: 845-851.
- Ballmer-Weber BK, Bircher A, Piletta P, Hofbauer GFL, Spring P, Anliker M, Gilardi S, Rast HP, Grillet JP, Simon D: Management of chronic hand eczema: Swiss consensus. Dermatol helvet 2012; in press.
- Diepgen TL, Elsner P, Schliemann S, Fartasch M, Köllner A, Skudlik C, John SM, Worm M; Deutsche Dermatologische Gesellschaft: Guideline on the management of hand eczema ICD-10 Code: L20. L23. L24. L25. L30. J Dtsch Dermatol Ges 2009; 7 Suppl 3: S1-16.
- Held E, Skoet R, Johansen JD, Agner T: The hand eczema severity index (HECSI): a scoring system for clinical assessment of hand eczema. A study of inter- and intraobserver reliability. Br J Dermatol 2005; 152: 302-307.
- Skudlik C, Dulon M, Pohrt U, Appl KC, John SM, Nienhaus A: Osnabrueck hand eczema severity index – a study of the interobserver reliability of a scoring system assessing skin diseases of the hands. Contact Dermatitis 2006; 55: 42-47.
- Hald M, Veien NK, Laurberg G, Johansen JD: Severity of hand eczema assessed by patients and dermatologist using a photographic guide. Br J Dermatol 2007; 156: 77-80.
- Boehm D, Schmid-Ott G, Finkeldey F, John SM, Dwinger C, Werfel T, Diepgen TL, Breuer K: Anxiety, depression and impaired health-related quality of life in patients with occupational hand eczema. Contact Dermatitis 2012; 67: 184-192.
- Mälkönen T, Alanko K, Jolanki R, Luukkonen R, Aalto-Korte K, Lauerma A, Susitaival P: Long-term follow-up study of occupational hand eczema. Br J Dermatol 2010; 163: 999-1006.
- Jensen JM, Scherer A, Wanke C, Bräutigam M, Bongiovanni S, Letzkus M, Staedtler F, Kehren J, Zuehlsdorf M, Schwarz T, Weichenthal M, Fölster-Holst R, Proksch E: Gene expression is differently affected by pimecrolimus and betamethasone in lesional skin of atopic dermatitis. Allergy 2012; 67: 413-423.
DERMATOLOGIE PRAXIS 2013; No. 1: 13-15.









