
Erythritol and xylitol are sugar alcohols that occur naturally in small quantities in berries and vegetables and are used as sweeteners in the food industry and can also be used by the pharmaceutical and cosmetics industries. When ingested as a sweetener, erythritol is quickly absorbed in the small intestine and excreted largely unchanged in the urine. In contrast, only 50% of xylitol is absorbed and metabolized in the liver, while the unabsorbed portion ends up in the large intestine. This partial absorption explains why the rapid ingestion of large amounts of xylitol can lead to osmotic diarrhea.
You can take the CME test on our learning platform after you have reviewed the recommended materials. Please click on the following button:
Xylitol and erythritol – physiology and metabolism
Erythritol and xylitol are sugar alcohols that occur naturally in small amounts in berries and vegetables and are used as sweeteners in the food industry and can also be used by the pharmaceutical and cosmetics industries [1–3]. When ingested as a sweetener, erythritol is rapidly absorbed in the small intestine and excreted largely unchanged in the urine [4]. In contrast, only 50% of xylitol is absorbed and metabolized in the liver, while the unabsorbed portion reaches the large intestine. This partial absorption explains why the rapid ingestion of large amounts of xylitol can lead to osmotic diarrhea. In the large intestine, xylitol is fermented by the intestinal microbiome. Numerous sugar alcohols (isomalt, lactitol, maltitol and xylitol) can positively influence the composition of the human intestinal microbiome. Xylitol promotes the formation of short-chain fatty acids such as butyrate and propionate [5,6]. Isomalt is metabolized by bifido bacterial strains, which also produce butyrate. Short-chain fatty acids, such as butyrate and propionate, supply the intestinal epithelium with energy and play an important role in maintaining the intestinal barrier [7]. Erythritol, on the other hand, which is only available to the large intestine to a limited extent due to its high absorption in the small intestine, appears to be hardly fermented. Long-term controlled studies in humans investigating the effect of regular consumption of sugar alcohols on the gut microbiome are still pending.
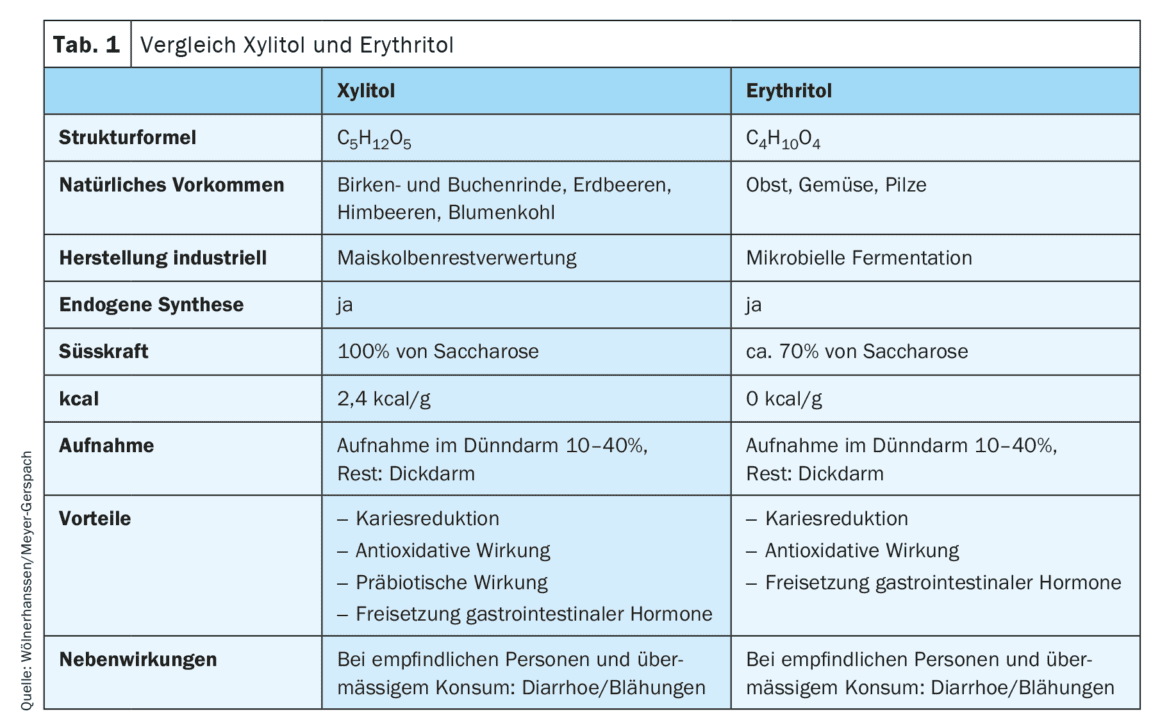
The oral flora is also positively influenced by the consumption of xylitol and erythritol. Caries-producing bacteria are reduced, salivary flow is stimulated and enamel mineralization is improved (Table 1). In the 1970s, in an elaborate study (Turku Study, Finland), 125 healthy volunteers were given all the confectionery they could consume ad libitum for two years. These were sweetened with either sucrose, fructose or xylitol. The subjects in the xylitol group consumed an average of approx. 65 g xylitol per day in this way (up to a maximum of 400 g xylitol per day). Apart from dose-dependent gastrointestinal complaints, no adverse events were observed [8]. Over the entire duration of the study, the xylitol group showed no significant increase in caries infestation, whereas new cases of caries occurred in the two sugar groups.
The two substances xylitol and erythritol are also attractive as sugar substitutes because the acute consumption of erythritol has no effect at all on plasma glucose and insulin levels, while xylitol only leads to a slight increase [9]. Recent studies have also repeatedly shown that acute consumption of erythritol and xylitol triggers the release of gastrointestinal satiety hormones (cholecystokinin [CCK], glucagon-like peptide-1 [GLP1] and peptide-tyrosine-tyrosine [PYY]), despite the absence or low number of calories [9,10]. After erythritol administration, a decrease in the hunger hormone ghrelin can also be observed [11]. No studies are yet available on the effect of xylitol on ghrelin levels. After ingestion of erythritol and xylitol, the release of gastrointestinal satiety hormones leads to a dose-dependent slowdown in gastric emptying – a satiety mechanism [9,10]. A central activation of brain networks involved in the regulation of appetite and reward can also be observed shortly after ingestion of the two substances [12]. Compared to beverages sweetened with sucralose or sucrose, a beverage sweetened with erythritol led to a significant reduction in energy intake during a subsequent ad libitum meal. The latter indicates the satiating effect of erythritol [13]. Data on the long-term effects of daily xylitol or erythritol consumption on calorie intake or body weight are not yet available.
Sugar alcohols and the metabolome
In addition to exogenous intake in small quantities from natural sources (e.g. berries, mushrooms, various vegetables) and through use as a sweetener, erythritol and xylitol – as well as other sugar alcohols (e.g. mannitol, sorbitol or ribitol) – are also produced endogenously by the human body [14]. For example, around 10 g of xylitol is synthesized endogenously every day. Under certain conditions, this endogenous production of sugar alcohols increases. The reasons for this are still largely unexplored. In a large epidemiological study of over 11,000 subjects using data from the EPIC-Norfolk cohort, it was found that the metabolites erythritol, ribitol, arabitol, xylitol and myo-inositol are associated with an increased risk of numerous diseases (e.g. kidney disease, heart failure, peripheral vascular disease, ischemic heart disease and stroke) [15]. Some studies suggest that higher fasting plasma concentrations of erythritol and xylitol are found in those at increased cardiovascular risk [16–18]. However, increased plasma concentrations of other sugar alcohols (e.g. arabitol, myo-inositol, threitol) and other metabolites have also been observed [17].
Interestingly, some studies also report a decrease in sugar alcohol concentrations in patients after weight loss. In the POUNDS-Lost study, higher levels of erythritol, mannitol, sorbitol, myo-inositol, arabitol and xylitol were associated with a higher risk of atherosclerotic cardiovascular disease and insulin resistance [19]. Weight loss led to a reduction in erythritol concentrations, which was associated with a decrease in fasting insulin and a decrease in blood lipid levels [19]. The randomized, controlled DiRECT** study also found that participants in the intervention group had lower levels of ribitol and erythritol [20].
** DiRECT = Diabetes Remission Clinical Trial
A major limitation of all these observational studies, which describe that sugar alcohols are elevated in certain diseases, is that they can only show associations and not causality. In addition, none of these studies investigated the exogenous intake of sugar alcohols that are also used as sweeteners. The origin of the sugar alcohols (exogenous intake or endogenous synthesis) is unclear. In certain historical cohorts, however, this classification is still possible: in a study published in 2019, serum samples from more than 3,500 patients collected prospectively towards the end of the 1980s were analyzed. It was also found that elevated erythritol levels at baseline were associated with an increased risk of developing coronary heart disease 30 years later [16]. However, erythritol was not approved for use as a sweetener in the food industry in the USA until 2001, and therefore the erythritol found in these blood samples collected 30 years earlier must have originated from endogenous synthesis. Theoretically, a small amount can also be obtained from natural sources (mushrooms, berries, vegetables).
It therefore remains unclear why the body’s own production of sugar alcohols is observed in certain diseases. One obvious explanation would be a connection with the blood glucose level, as glucose is the substrate for endogenous sugar alcohol synthesis and numerous metabolic diseases are ultimately associated with a dysregulation of glucose metabolism. In the mouse model, chronic administration of sugar leads directly to increased endogenous erythritol production [21]. This hypothesis is contradicted by the fact that the association between higher erythritol concentrations and cardiovascular risk in a recently published study was independent of whether the cohorts were stratified into patients with high or low blood glucose or with/without diabetes [17]. Another hypothesis points to the antioxidant properties of numerous sugar alcohols [22]. In vitro experimentsindicate that oxidative stress stimulates the production of sugar alcohols such as sorbitol, L-arabitol, xylitol or dulcitol. It is possible that the increased production of sugar alcohols associated with elevated blood glucose levels and oxidative stress is a kind of “rescue attempt” by the body to both rapidly lower glucose levels and counteract oxidative stress. Given the increasing consumption of erythritol and xylitol in recent years in people with obesity and/or diabetes and thus increased cardiovascular risk, future observational studies should also consider the possibility of reverse causality: Patients with a corresponding risk profile might be more inclined to resort to sugar alcohols as sugar substitutes.
In summary, although elevated circulating plasma concentrations of erythritol, xylitol and other sugar alcohols may be associated with various diseases, the underlying cause is currently unclear. Future studies aiming to further investigate the association of these metabolites with various diseases should definitely take into account the dietary habits of the participants (i.e. consumption of erythritol and xylitol as sweeteners, but also intake from natural sources).
Sugar alcohols and cardiovascular risk
Long-term excessive sugar consumption leads to high blood pressure, weight gain, insulin resistance, diabetes, dyslipidemia and fatty liver disease and thus contributes to an increase in cardiovascular risk. Both acute and chronically elevated blood glucose levels also promote a prothrombotic state, both in diabetics and non-diabetics [23]. Patients with diabetes and healthy individuals are therefore advised to keep their blood sugar levels as low as possible and to limit their sugar consumption. Replacing sugar with various alternatives can at least partially contribute to achieving this goal.
Important factors that influence vascular health and promote the development of cardiovascular disease are hyperglycemia and the resulting oxidative stress. The beneficial effects of oral xylitol and erythritol administration on glucose metabolism have been repeatedly observed in diabetic and non-diabetic rats [24]. The antihyperglycemic effects can be explained by various mechanisms such as inhibition of alpha-amylase and alpha-glucosidase, significantly delayed gastric emptying and reduced glucose absorption in the small intestine. Glucose uptake in the periphery – e.g. in muscle tissue – is also increased [25,26]. Even tropic effects on the islet cells in the pancreas have been observed in diabetic rats given xylitol and erythritol. In humans, acute ingestion of erythritol and xylitol also delays gastric emptying [27]. In patients with obesity, however, the daily intake of 36 g erythritol or 24 g xylitol over a period of 5-7 weeks had no effect on glucose absorption in the small intestine [28].
In vitro testsshow that erythritol – and other sugar alcohols – are strong hydroxyl radical scavengers and can therefore be beneficial for the endothelium [22]. In a diabetic rat model, administration of erythritol prevented endothelial dysfunction. In a pilot study in patients with diabetes, vascular function was also examined after acute (i.e. 2 hours after 24 g erythritol) and chronic (36 g/day over four weeks) erythritol consumption. After acute administration, the endothelial function of the small vessels improved and when administered over four weeks, aortic stiffness decreased (reduced central pulse pressure) [29]. In a randomized controlled trial in normoglycemic patients with obesity, however, no statistically significant effects of daily erythritol or xylitol intake over 5 weeks on vascular function were observed [30]. The discrepancy between these two in vivo human studiescould be due to differences in diabetic status. Since erythritol appears to act as an antioxidant, it is possible that an effect is only observed in hyperglycemic patients.
In the context of vascular health, it is also worth noting that xylitol and erythritol appear to have an effect on collagen. A study in healthy and diabetic rats showed that xylitol intake increased the hydroxyproline content measured in the skin and led to a decrease in hexose content and collagen fluorescence, suggesting that xylitol has a positive effect on both collagen synthesis and glycosylation [31]. In vitro experimentsalso suggest a collagen-stabilizing effect of both xylitol and erythritol. Whether these substances are also able to positively influence vascular collagen and whether this effect can also be found in vivo in humans has not yet been investigated.
As already described, there is an association between increased plasma erythritol and xylitol concentrations and an increased risk of cardiovascular events, whereby the increased levels are likely to originate primarily from autosynthesis. In addition, a research group recently postulated that these two substances may also directly promote the development of cardiovascular disease by influencing platelet reactivity [17,18,32]. In their publications, this research group presented data from various substudies: in vitro testson human platelets exposed to erythritol or xylitol, in vivo coagulation testsin a mouse model and ex vivo datafrom platelet stimulation tests on healthy humans who had acutely ingested xylitol or erythritol. In vitro platelet stimulation testsare of limited value and cannot be easily transferred to in vivo conditionsin the human body. For example, the increased osmolarity can influence intracellular signal transmission in the platelets – an unspecific effect [33]. Even findings from animal models (mouse model) cannot be transferred 1:1 to humans. However, the species mice and rats appear to tolerate xylitol and erythritol well over a longer period of time at higher doses: the use of feed containing up to 20% xylitol or erythritol and administered over 2 years (i.e. over the entire lifespan) did not lead to cardiovascular changes and did not result in a shortened lifespan [34,35].
Finally, in the ex vivo platelet stimulation test, ten healthy volunteers were administered either 30 g xylitol, 30 g erythritol or 30 g glucose per os and the platelet response to ex vivo stimulationwith TRAP6 and ADP was examined once before and once 30 minutes after ingestion [18,32]. In these studies, increased platelet reactivity was observed after ingestion of xylitol and erythritol, while glucose had no effect. However, with 10 subjects in each group, the human studies were small; there was no placebo arm, and only a single time point (30 min) after ingestion was studied. Due to the parallel design, it is also not possible to directly compare the effects of the three sweeteners in the same person. Although the described increase in platelet reactivity was statistically significant, the question arises as to its clinical relevance. There are numerous environmental influences that affect platelet reactivity in the short term and are more likely to be interpreted as natural fluctuations without health consequences.
Acute physical activity temporarily increases the tendency to aggregate. After food intake, both a reduction and an increase in the tendency to aggregate are described in the literature [36,37]. Thus, while the results from the pilot study warrant further investigation, it is not clear at this time whether the findings can be replicated in larger placebo-controlled, randomized trials, whether the described effect is only a short-term phenomenon (as with other postprandial observations), and whether the effect is also found in vivo (and not only with ex vivo stimulation).
Summary
The harmful effects of chronic overconsumption of conventional sugar are well documented. High blood sugar levels have a negative effect on vascular health and also promote platelet aggregation, among other things. Reducing sugar consumption is important for patients with diabetes as well as for healthy people. Sugar alcohols can be used to at least partially replace sugar in the diet. The consumption of erythritol and xylitol stimulates the release of gastrointestinal satiety hormones, while the effects on blood glucose and insulin concentrations remain minimal. These effects are desirable in terms of metabolic and cardiovascular health. A possible short-term effect of xylitol and erythritol on the aggregation tendency of human platelets has so far been observed in a small pilot study ex vivo. These results need to be replicated in placebo-controlled studies with larger samples and longer duration after ingestion.
Long-term studies on the regular consumption of large amounts of sugar alcohols are limited and there is still a need for carefully designed studies in this area. However, based on current knowledge, the evidence for adverse effects of regular table sugar on cardiovascular health is much stronger than that for potential risks from erythritol or xylitol. The causes and significance of increased endogenous synthesis of sugar alcohols in connection with various diseases must be investigated further.
Take-Home-Messages
- Chronically high blood sugar levels damage vascular health and promote platelet aggregation, among other things. A reduction of sugar consumption is essential for people with diabetes and healthy individuals.
- Sugar alcohols such as erythritol and xylitol can partially replace sugar. They have little effect on blood sugar and insulin, but stimulate the release of gastrointestinal satiety hormones and may have prebiotic properties – a potential benefit for metabolic health.
- Long-term studies on the regular consumption of large quantities of sugar alcohols are lacking. There is a need for research here.
- The increased endogenous production of sugar alcohols, for example in cardiovascular diseases and diabetes, should be investigated further.
- Pilot studies indicate a possible short-term effect of xylitol and erythritol on platelet aggregation. These findings need to be verified in larger, placebo-controlled studies.
Literature:
- de Cock P, et al: Erythritol Is More Effective Than Xylitol and Sorbitol in Managing Oral Health Endpoints. Int J Dent 2016; 2016: 9868421.
- Mäkinen KK, Söderling E: A quantitative study of mannitol, sorbitol, xylitol, and xylose in wild berries and commercial fruits. J Food Sci 1980; 45: 367-371.
- Ahuja V, et al: Biological and Pharmacological Potential of Xylitol: A Molecular Insight of Unique Metabolism. Foods 2020; 9(11).
- Bordier V, et al: Absorption and Metabolism of the Natural Sweeteners Erythritol and Xylitol in Humans: A Dose-Ranging Study. Int J Mol Sci 2022. 23(17).
- Makelainen HS, et al: The effects of polydextrose and xylitol on microbial community and activity in a 4-stage colon simulator. J Food Sci 2007; 72(5): M153-159.
- Sato T, et al: Prebiotic potential of L-sorbose and xylitol in promoting the growth and metabolic activity of specific butyrate-producing bacteria in human fecal culture. FEMS Microbiol Ecol 2017; 93(1).
- Mohamed Elfadil O, et al: Butyrate: More Than a Short Chain Fatty Acid. Curr Nutr Rep 2023; 12(2): 255-262.
- Mäkinen KK, Scheinin A: Turku sugar studies VI. The administration of the trial and the control of the dietary regimen. Acta Odontologica Scandinavica 1975; 33: 105-127.
- Wolnerhanssen BK, et al: Gut hormone secretion, gastric emptying, and glycemic responses to erythritol and xylitol in lean and obese subjects. Am J Physiol Endocrinol Metab 2016; 310(11): E1053-1061.
- Wolnerhanssen BK, et al: Gastric emptying of solutions containing the natural sweetener erythritol and effects on gut hormone secretion in humans: A pilot dose-ranging study. Diabetes Obes Metab 2021; 23(6): 1311-1321.
- Teysseire F, et al: Metabolic Effects and Safety Aspects of Acute D-allulose and Erythritol Administration in Healthy Subjects. Nutrients 2023; 15(2).
- Meyer-Gerspach AC, et al: Erythritol and xylitol differentially impact brain networks involved in appetite regulation in healthy volunteers. Nutr Neurosci 2022; 25(11): 2344-2358.
- Teysseire F, et al: Oral Erythritol Reduces Energy Intake during a Subsequent ad libitum Test Meal: A Randomized, Controlled, Crossover Trial in Healthy Humans. Nutrients 2022; 14(19).
- Hootman KC, et al: Erythritol is a pentose-phosphate pathway metabolite and associated with adiposity gain in young adults. Proc Natl Acad Sci U S A 2017; 114(21): E4233-E4240.
- Pietzner M, et al: Plasma metabolites to profile pathways in noncommunicable disease multimorbidity. Nat Med 2021; 27(3): 471-479.
- Wang Z, et al: Metabolomic Pattern Predicts Incident Coronary Heart Disease. Arterioscler Thromb Vasc Biol 2019; 39(7): 1475-1482.
- Witkowski M, et al: The artificial sweetener erythritol and cardiovascular event risk. Nat Med 2023; 29(3): 710-718.
- Witkowski M, et al: Xylitol is prothrombotic and associated with cardiovascular risk. Eur Heart J 2024.
- Heianza Y, et al: Abstract: Changes in Plasma Levels of Nonnutritive Sweetener Erythritol Are Related to Two-Year Changes of Insulin Sensitivity in Response to Weight-Loss Diets – The POUNDS Lost trial. Diabetes Care 2023; 72 (Supplement_1): 48-LB.
- Corbin LJ, et al: The metabolomic signature of weight loss and remission in the Diabetes Remission Clinical Trial (DiRECT). Diabetologia 2024; 67(1): 74-87.
- Ortiz SR, Field MS: Sucrose Intake Elevates Erythritol in Plasma and Urine in Male Mice. J Nutr 2023; 153(7): 1889-1902.
- den Hartog GJ, et al: Erythritol is a sweet antioxidant. Nutrition 2010; 26(4): 449-458.
- Vaidyula V, et al: Platelet and monocyte activation by hyperglycemia and hyperinsulinemia in healthy subjects. Platelets 2006; 17(8): 577-585.
- Islam MS, Indrajit M: Effects of xylitol on blood glucose, glucose tolerance, serum insulin and lipid profile in a type 2 diabetes model of rats. Ann Nutr Metab 2012; 61(1): 57-64.
- Chukwuma CI, Islam MS: Effects of xylitol on carbohydrate digesting enzymes activity, intestinal glucose absorption and muscle glucose uptake: a multi-mode study. Food Funct 2015; 6(3): 955-962.
- Chukwuma CI, et al: Erythritol reduces small intestinal glucose absorption, increases muscle glucose uptake, improves glucose metabolic enzymes activities and increases expression of Glut-4 and IRS-1 in type 2 diabetic rats. Eur J Nutr 2018; 57(7): 2431-2444.
- Woelnerhanssen BK, et al: Gut hormone secretion, gastric emptying and glycemic responses to erythritol and xylitol in lean and obese subjects. Am J Physiol Endocrinol Metab 2016; ajpendo 00037 2016.
- Bordier V, et al: Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity. Nutrients 2021; 13(11).
- Flint N, et al: Effects of erythritol on endothelial function in patients with type 2 diabetes mellitus: a pilot study. Acta Diabetol 2014; 51(3): 513-516.
- Bordier V, et al: Effects of a 5-week intake of erythritol and xylitol on vascular function, abdominal fat and glucose tolerance in humans with obesity: a pilot trial. BMJ Nutr Prev Health 2023; 6(2): 264-272.
- Knuuttila ML, et al: Effects of dietary xylitol on collagen content and glycosylation in healthy and diabetic rats. Life Sci 2000; 67(3): 283-290.
- Witkowski M, et al: Ingestion of the Non-Nutritive Sweetener Erythritol, but Not Glucose, Enhances Platelet Reactivity and Thrombosis Potential in Healthy Volunteers. Arterioscler Thromb Vasc Biol 2024.
- Sudic D, et al: High glucose levels enhance platelet activation: involvement of multiple mechanisms. Br J Haematol 2006; 133(3): 315-322.
- Hunter B, et al: Xylitol Tumorigenicity and Toxicity Study in Long-Term Dietary Administration To Rats (Final Report). Huntingdon Research Centre, Huntingdon, Cambridgeshire, England. F. Hoffman La Roche Company, Ltd, Basel, Switzerland 1978; 11-14: 2250.
- Lina BA, et al: Chronic toxicity and carcinogenicity study of erythritol in rats. Regul Toxicol Pharmacol 1996; 24: S264-279.
- Gow IF, et al: High sodium intake increases platelet aggregation in normal females. J Hypertens Suppl 1987; 5(5): S243-246.
- Ahuja KD, et al: Postprandial platelet aggregation: effects of different meals and glycemic index. Eur J Clin Nutr 2012; 66(6): 722-726.
HAUSARZT PRAXIS 2025; 20(1): 12–16
| Sources of funding/conflicts of interest Bettina Wölnerhanssen is supported by the SNSF (Swiss National Science Foundation; grant no.: CRSII5_186346 and 320030E_189329) and the Botnar Foundation. Anne Christin Meyer-Gerspach is supported by the SNSF (Swiss National Science Foundation; grant no.: 320030E_189329) and the Uniscientia Foundation. The authors confirm that there are no conflicts of interest. |









