Case Report: A 44-year-old male patient presented with severe neck and occipital headache, increased in flexion/rotation, also progressive neck and swallowing pain. Laboratory findings included leukocytosis (13,000× 109/l) and CRP elevation (52.2 mg/l). However, with primary suspicion of meningitis, CSF analysis showed no abnormalities. Nearly refractory neck and head pain (despite adapted pain therapy) was followed by MRI of the skull with age-matched intracranial findings but evidence of a partially captured T2 hyperintense process retropharyngeally.
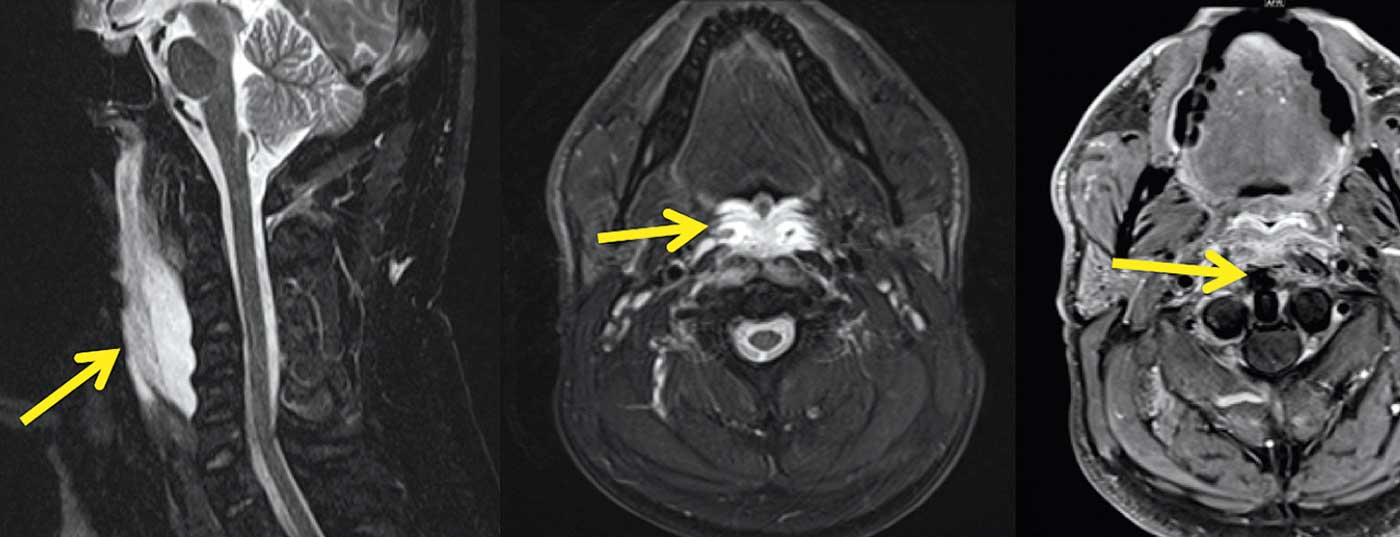
Pharyngo-laryngoscopy revealed no evidence of local infection, but swallowing reflexes were absent on pain provocation at the posterior pharyngeal wall. Subsequent MRI of the neck demonstrated a distinct signal change in the longus colli muscle with a long-distance, spindle-shaped T2w hyperintense formation between the longus colli muscle and the posterior pharyngeal wall (Fig. 1A) without diffusion restriction and with moderate, marginal contrast uptake. Furthermore, edema of the posterior pharyngeal wall including mucosa was present (arrow in Fig. 1B) as well as rather minor signal changes of the adjacent soft tissues. There was no abnormal lymphadenopathy. These findings were rather against a retropharyngeal abscess, which could also be excluded by means of local puncture (little serous fluid without evidence of germs). With regular signal from the cervical vertebral bodies, spondylodiscitis was also unlikely to be the cause of retropharyngeal collection.
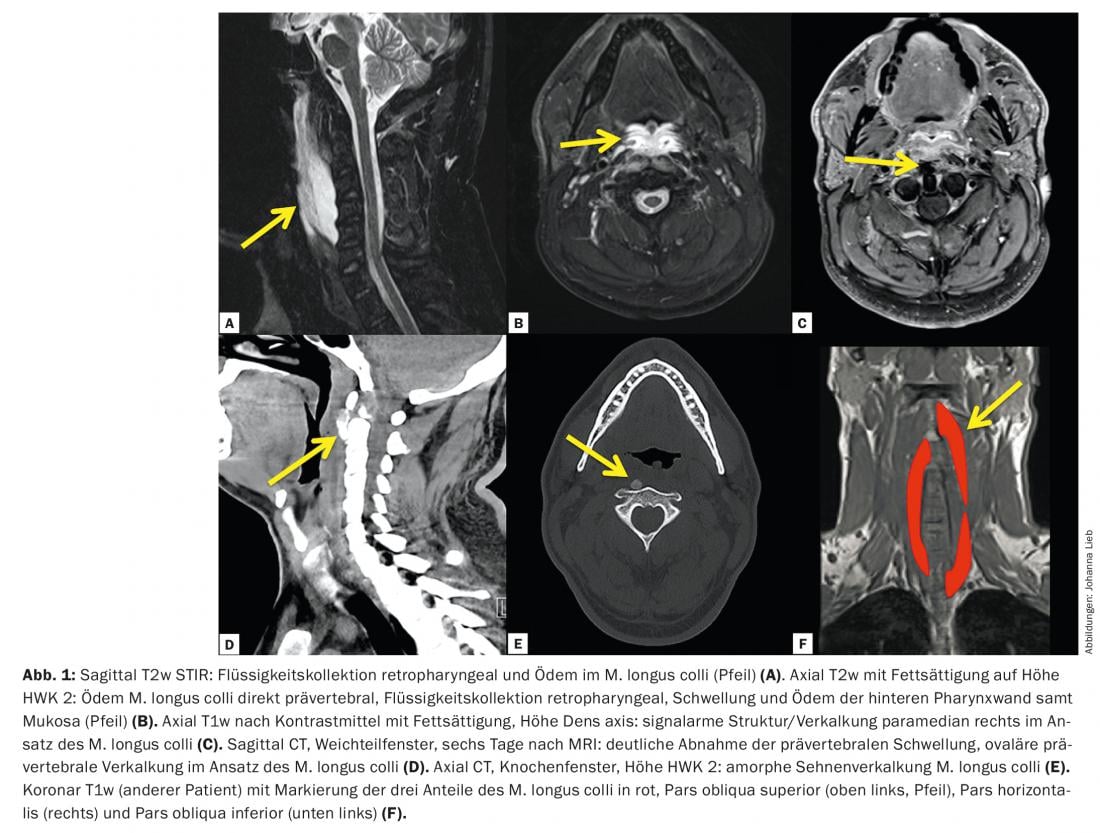
In T1w and T2w, low-signal structures were found in the tendon insertion of the longus colli muscle at the anterior tuberosity of the atlas (arrow in Fig. 1C), This led to the suspected diagnosis of rare acute calcifying tendinitis of the longus colli muscle, which was confirmed by neck CT during the course of the study.
Amorphous calcifications in the tendon of the longus colli muscle (Fig. 1C-E) are pathognomonic for this clinical picture. Under several days of steroid therapy and subsequent therapy with anti-inflammatory drugs, the tendinitis clearly regressed, as did the patient’s complaints.
Clinical picture: The clinical picture was first described in 1964 [1]. In the meantime, several case reports exist. Similar to the above example, affected patients complain of often subacute onset occipital headache, neck pain, neck stiffness, sore throat, and fever [2]. These symptoms initially suggest meningitis, subarachnoid hemorrhage, spondylodiscitis, or retropharyngeal abscess. Laboratory parameters are mostly nonspecific, with occasional mild to moderate elevation of inflammatory signs. Swallowing difficulties follow over the course of days. The typical patient age is the third to sixth decade of life, and women and men are equally affected.
One possible cause of calcifying tendinitis of the longus colli muscle is calcium pyrophosphate dihydrate deposition disease (CPPD), which is characterized by deposition of calcium phosphates in periarticular tissues (predominantly in tendons) and mainly affects the shoulder, hip, hand, and ankle joints. The exact etiology of CPPD is unknown, but post-traumatic (or repeated trauma), necrotic, ischemic, and metabolic pathomechanisms are discussed [3]. In rare cases, CPPD may involve the longus colli muscle.
The M. longus colli consists of three parts, pars obliqua superior, pars recta, and pars obliqua inferior(Fig. 1F). In calcifying tendinitis, the fibers of the pars obliqua superior (arrow in Fig. 1F) with attachment to the tuberculum anterius atlantis affected with typical calcifications leading to the diagnosis. In the case shown, there is a pronounced retropharyngeal effusion, but this can also be much narrower and manifest only as a retropharyngeal fluid track a few millimeters wide. Common to all cases are the pathognomonic tendon attachment calcifications.
Discussion: Calcifying tendinitis of the longus colli muscle is a rare but important differential diagnosis to retropharyngeal abscess in neck pain with retropharyngeal effusion. In particular, pathognomonic calcifications in the tendon attachment to the anterior atlantal tuberosity and the absence of concomitant reactions (phlegmon, lymphadenopathy) help in making the diagnosis and in avoiding major invasive procedures. Acute calcifying tendinitis of the longus colli muscle is treated conservatively with NSAIDs and heals after a few weeks.
Literature:
- Hartley J: Acute Cervical Pain associated with Retropharyngeal Calcium Deposit. A Case Report. The Journal of Bone and Joint Surgery 1964; 46(A): 1753-1754.
- Offiah CE, Hall E: Acute calcific tendinitis of the longus colli muscle: Spectrum of CT Appearances and Anatomical Correlation. The British Journal of Radiology 2009; 82(978): e117-121, doi:10.1259/bjr/19797697.
- Hayes CW, Conway WF: Calcium hydroxyapatite deposition disease. Radiographics: A Review Publication of the Radiological Society of North America 1990; 10(6): 1031-1048, doi:10.1148/radiographics.10.6.2175444.
Further reading:
- Eastwood JD, Hudgins PA, Malone D: Retropharyngeal effusion in acute calcific prevertebral tendinitis: diagnosis with CT and MR imaging. AJNR Am J Neuroradiol 1999; 19(9): 1789-1792.
- Chung T, Rebello R, Gooden EA: Retropharyngeal calcific tendinitis: case report and review of literature.
- Emerg Radiol 2005; 11(6): 375-380.
- Hviid C, et al: Retropharyngeal tendinitis may be more common than we think: a report on 45 cases seen in Danish chiropractic clinics. J Manipulative Physiol Ther 2009; 32(4): 315-320.
- Ellika SK, et al: Acute calcific tendinitis of the longus colli: an imaging diagnosis. Dentomaxillofac Radiol 2008; 37(2): 121-124.
InFo NEUROLOGY & PSYCHIATRY 2016; 14(1): 36-37.