41% of the Swiss population is overweight. The Swiss Diabetes Association estimates that nearly 500,000 people in Switzerland have diabetes. Insulin-resistant obese diabetics are at increased risk for an army of chronic diseases. A critical investigation of the causes of these circumstances and their interrelationships.
Charles Darwin is often attributed this quote: “It is not the strongest of the species that survives, nor the most intelligent. It is the one that is the most adaptable to change.”
In his original 1859 “On the Origin of Species” the quotation is effectively not found, but the following statement: “Whatever the cause may be of each slight difference in the offspring from their parents – and a cause for each must exist – it is the steady accumulation, through natural selection, of such differences, when beneficial to the individual, that gives rise to all the more important modifications of structure, by which the innumerable beings on the face of this earth are enabled to struggle with each other, and the best adapted to survive.”
Be that as it may, adaptation or adaptability seems to be effectively a crucial prerequisite for surviving inhospitable or destructive environmental changes in a healthy way. But adaptation takes a lot of time.
The twin diseases obesity and diabetes
According to the 2012 Swiss Health Survey, 41% of the population is overweight, 51% of men and 32% of women. In terms of full-blown obesity, the differences between men and women are less pronounced (11 versus 9%). Within 20 years, the percentage of obese people has almost doubled. For men, it increased from 6% to 11%; for women, from 5% to 9%. The 15- to 24-year-olds are particularly affected by this increase [1].
The Swiss Diabetes Association reports alarming figures [2]. It estimates that nearly 500,000 people in Switzerland have diabetes, of which about 40,000 are type 1 diabetics. Worldwide, 415 million people have diabetes, which represents about 5.6% of the world’s population. China leads with about 109, India with 69, the U.S. with 29, Brazil with 14 and Russia with 12 million diabetics. According to estimates by the International Diabetes Federation, around 642 million people worldwide will have diabetes by 2040, which means one in ten people.
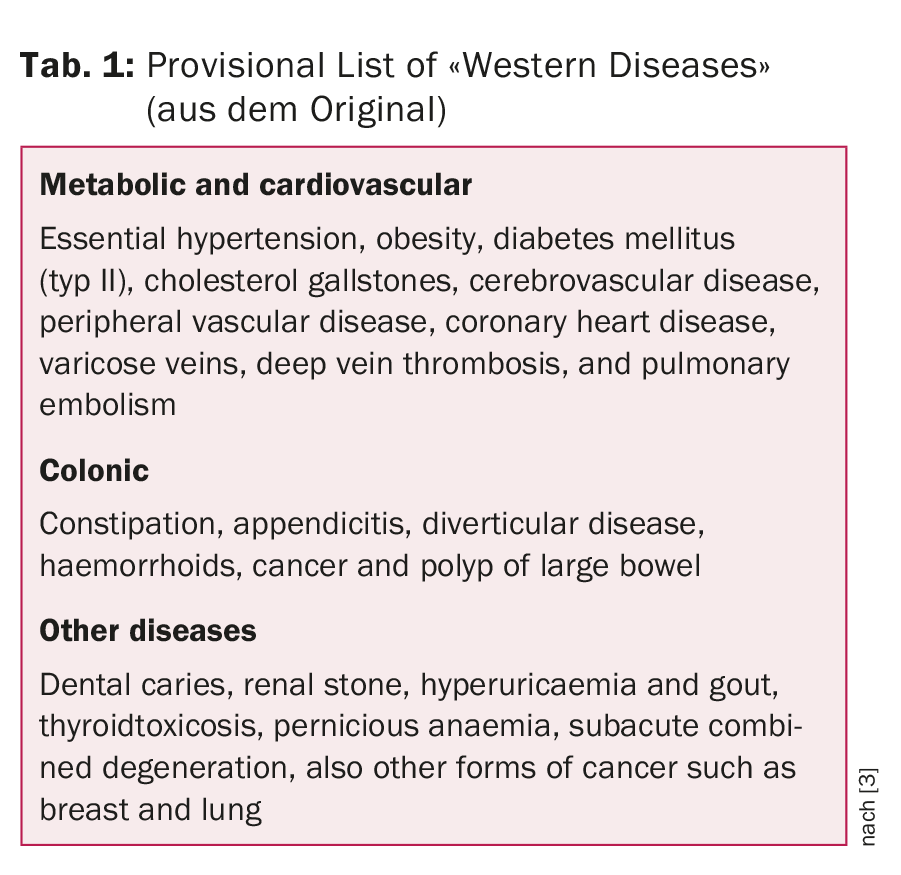
The second half of the 19th century saw an epidemic increase in obesity and type 2 diabetes in Western populations, and more recently in Asian and indigenous populations, which are now some of the dominant diseases of the modern era. Insulin resistance plays an important role in both diseases. Insulin-resistant obese diabetics are at increased risk for an army of chronic diseases. Table 1 lists the “Western Diseases” described by Burkitt & Trowell and associated with insulin resistance.
How can these observations be explained? What allowed such a serious epidemic to develop?
The metabolic-vascular syndrome
Lechner et al. summarize the nutritional recommendations in metabolic-vascular syndrome in a very readable review [4]. They postulate that metabolic syndrome, cardiovascular disease, nonalcoholic fatty liver disease (NAFLD), and the most common cancers (colon, breast, and prostate) share common causes and group them together as the “metabolic-vascular syndrome.” Insulin resistance, which is associated with compensatory hyperinsulinemia, is thought to play a central role pathophysiologically. Gary Taubes, in his book “The Case Against Sugar” [5], describes the ultimate “if/then” hypothesis: “If these Western diseases are associated with obesity, diabetes, insulin resistance, and metabolic syndrome, which many of them are, then whatever causes insulin resistance and metabolic syndrome is likely to be the necessary dietary trigger for the diseases, or at least a key player in the causal pathway.”
Fat reduction recommendations
Because of the increase in cardiovascular disease, authorities in the United States in 1977 and in England in 1983 introduced dietary recommendations, both of which focused on dietary fat restriction. Specifically, based on Ancel Key’s fat hypothesis, a reduction in total fat intake to <30 energy percent, saturated fat to <10 energy percent, and cholesterol to <300 mg/day was recommended. This compensatorily led to a higher intake of starch- and sugar-rich foods [4]. There was no scientific evidence to support the introduction of this “Step 1 Diet” for 220 million Americans and 56 million English people [6]. Ancel Keys, in a careful analysis of the literature and his own controlled metabolic study, came to the following conclusion in 1956 [7]: “It is concluded that in adult men the serum cholesterol level is essentially independent of the cholesterol intake over the whole range of natural human diets.”
Dietary cholesterol is now also classified as a safe nutrient in the latest U.S. Dietary Guidelines and, contrary to popular belief, the level of total fat intake is not a risk factor for the development of metabolic-vascular disease [8,9]. In an analysis of the recently published PURE study (Prospective Urban Rural Epidemiology, [10]), which examined the dietary habits of 135,335 people from 18 countries on five continents, a diet high in fat was associated with the lowest mortality risk. High carbohydrate content, on the other hand, was associated with higher all-cause mortality. Of note, this large cohort study of 35-70 year olds with no previous cardiovascular disease was the first to examine low-income countries. When studying the literature on fat, these findings are not surprising, and so the authors’ suggestion that global dietary guidelines should be reconsidered in light of these findings is not surprising.
Refined sugar – the main suspect
Gary Taubes argues in his book that increasing consumption of sugar and “high-fructose corn syrup” (corn syrup, glucose-fructose syrup) is the nutrient trigger responsible for “Western diseases,” a variety of chronic diseases. Peter Cleave reported as early as 1950 on what he called “saccharine disease”: the alarming increase in tooth decay provided an obvious key to explaining the causes of “Western diseases.” “It would be an extraordinary coincidence,” he wrote, “if these refined carbohydrates, which are known to wreak such havoc on the teeth, did not also have profound repercussions on other parts of the alimentary canal during their passage along it, and on other parts of the body after absorption from the canal.”
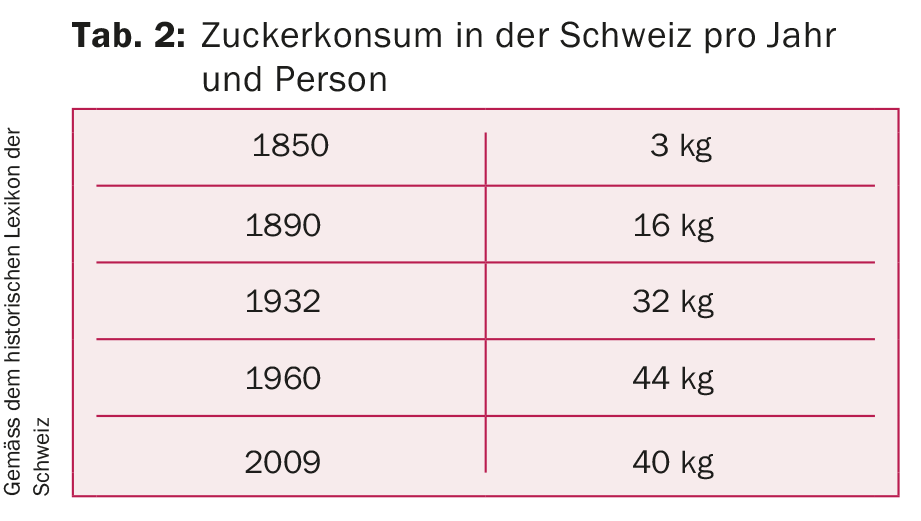
The consumption of refined sugar in Switzerland has increased more than thirteenfold in 150 years (Tab. 2). According to Gastromed Suisse, the Swiss consumed as much as 52 kg of sugar per capita in 2014/2015 [11].
In evolutionary terms, 150 years is a very short period of time for adaptation processes in the organism. The epidemic spread of chronic diseases based on excess carbohydrate intake and poor carbohydrate quality combined with today’s widespread muscular inactivity, which contribute to insulin resistance [12], now affect almost all populations in the world.
Sugar metabolism
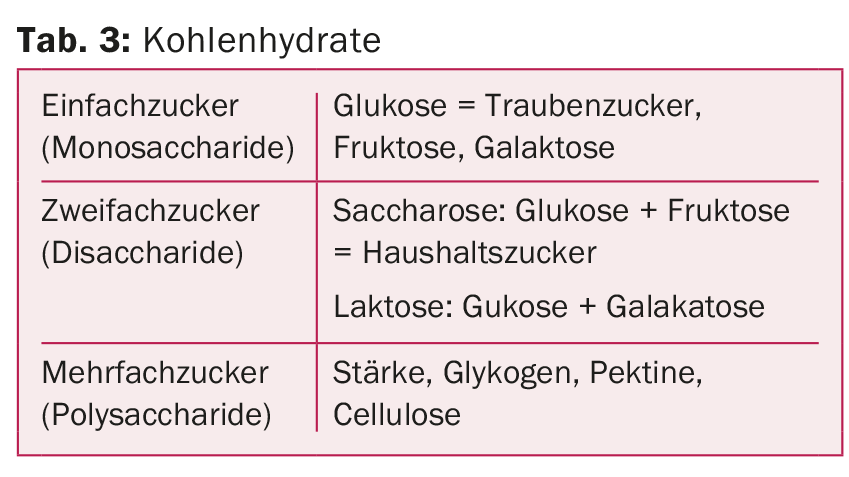
Digestible carbohydrates provide the body with monosaccharides for energy production, and the non-digestible carbohydrates are available for fermentation in the colon by intestinal bacteria (Tab. 3) . Dietary fibers interact with the intestinal “microbiota”, reduce inflammation and thus have a beneficial effect on lipid metabolism. The monosaccharide glucose can be absorbed by every cell in the body and burned for energy. As long as we don’t overeat permanently, glucose won’t be a problem either. Fructose, on the other hand, is absorbed almost exclusively in the liver . Glucose, lactate and fatty acids are produced in the degradation process. Diets high in fructose may increase hepatic de novo lipogenesis and plasma triglyceride concentrations.
Carbohydrate quality
Lechner et al. [4] state in their article that carbohydrate quality is of outstanding importance in relation to metabolic-vascular risk. It influences – partly in a calorie-independent manner – endocrine signals such as hunger and satiety, hepatic de novo lipogenesis, the central reward system, and the intestinal microbiome. Carbohydrate intake from processed foods high in added sugars and refined starches has a significantly more insulinogenic effect than carbohydrate intake from natural foods, which are generally rich in fiber. A good marker for assessing carbohydrate quality is the quotient of carbohydrates and fiber content (dietary fiber). A ratio <5:1 indicates very high quality carbohydrate sources, while a ratio of >10:1 indicates non-recommended carbohydrate sources.
Carbohydrate quality and digestibility may influence postprandial plasma glucose concentration and inflammatory response, which may promote the development of insulin resistance, metabolic syndrome, and type 2 diabetes, depending on carbohydrate intake volume. Foods with a high glycemic index (GI) and high glycemic load (GL) are associated with an increased risk of “Western Diseases” following the above. Reducing GI and GL improves metabolic control, increasing protein to carbohydrate ratio reduces glycemia, inflammation can be mitigated by dietary modifications [12].
From the metabolically healthy to the metabolically ill
Intrahepatic lipid content is associated with the development of type 2 diabetes as well as atherogenic dyslipidemia (low HDL, high triglycerides). Over-demand intake of certain carbohydrates results in increased hepatic de novo lipogenesis and increased “output” of triglyceride-rich VLDL particles from the liver, which supply all tissues with essential fats, cholesterol, and antioxidants. Triglycerides are increasingly stored ectopically in visceral organs after exhaustion of the storage capacity of expanding adipocytes. Hypertrophy of adipocytes is in turn associated with accumulation of macrophages in white adipose tissue, which eventually leads to adipocyte death with increased release of proinflammatory cytokines. In a vicious circle, this leads to an increase in fatty liver disease (NAFLD), which promotes insulin resistance. An excess of glucose and fructose in the blood leads to glycation damage of proteins, which can no longer perform their function. Over time, the accumulation of glycated “protein debris” (advanced glycation end products, AGEs) occurs. These play a critical role in certain aging processes, atherosclerosis, and long-term consequences of type 2 diabetes [13]. This negative spiral is described by Seneff et al. [13] increased in a diet low in fat and cholesterol but high in fructose.
An insulin resistance of the liver represents a massive disturbance of the entire metabolism of carbohydrates. The body secretes too much insulin and yet can no longer vary blood glucose levels as needed. This not only promotes the development of type 2 diabetes, but can also lead to obesity and, in the course of time, to hypertension and the typical atherogenic dyslipidemia with an excess of triglycerides and low HDL. If all this comes together, we speak of the metabolic syndrome. These developments can be a basis on which many of the “Western Diseases” can develop particularly early and quickly.
Too much food and too little exercise, are often promoted as causes for the alarming increase in “Western Diseases”. Based on what has been described, couldn’t a much simpler and more likely answer be true – sugar?
What dietary patterns should mannun recommend
An optimal dietary strategy or healthy eating patterns should maintain health and be primarily prophylactic against chronic disease. Ideally, they should fit metabolically healthy individuals, preventing progression from subclinical metabolic changes to manifest disease while providing optimal therapy for those already ill.
The best evidence-based nutritional strategy for the prevention and treatment of diabetes mellitus should reduce postprandial glycemia and insulinemia without having negative effects on other risk factors. Healthy Mediterranean dietary patterns and low-GI/GL diets (e.g., vegetarian diets) may be recommended in place of conventional low-fat diets.
Conclusions
Healthy eating must automatically lead to a balanced and lower-energy nutrient intake without calorie counting. But the “right diet” should fulfill many other requirements: It should be enjoyable, implementable without prohibitions, versatile, tasty, sensual, adaptable to socio-cultural and individual habits, suitable for young and old, healthy and sick, and evidence-based.
The Mediterranean diet is recommended as a prime example of a healthy diet, as it has been shown to significantly reduce heart attack mortality [14] and is associated with reductions in all-cause and cancer mortality [15].
Ultimately, it’s about a healthy lifestyle that focuses not on food, but on enjoying it in moderation. The question remains open whether the Mediterranean lifestyle is in itself good for health. Why don’t we reintroduce the siesta and leave the hustle and bustle of everyday life behind? For as an old German proverb says, “To have lived merrily and died blessedly is to have spoiled the devil’s reckoning.”
Take-Home Messages
- Good food quality has a beneficial effect on metabolic-vascular risk.
- If insulin resistance is present, reducing the glycemic load is the most useful nutritional therapeutic measure.
- Calorie counting and focus on isolated nutrients are out.
- Adaptation of Mediterranean dietary patterns has been shown to significantly reduce myocardial infarction mortality and is associated with reductions in all-cause and cancer mortality.
The author has no financial dependencies related to the article
Literature:
- Swiss Federal Statistical Office: Swiss Health Survey 2012. www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/erhebungen/sgb.html
- DiabetesSwitzerland: Facts + Figures. www.diabetesschweiz.ch/diabetes/facts-figures/
- Hugh Trowell and Denis Burkitt, Western Diseases: Their Emergence and Prevention, 1981.
- Lechner K, et al: Nutritional recommendations in metabolic-vascular syndrome. Dtsch Med Wochenschr 2017; 142: 1613-1626.
- Gary Taube: The Case Against Sugar. First edition. Knopf, New York, 2016.
- Harcombe Z, et al: Evidence from randomized controlled trials did not support introduction of dietary fat guidelines in 1977 and 1983: a systematic review and metaanalysis. Open Heart 2015; 2: e000196.
- Keys A, et al.: Diet and serum cholesterol in man. Lack of effect of dietary cholesterol. J Nutr 1956; 59(1): 39-56.
- Mozaffarian D, Ludwig DS: The 2015 US Dietary Guidelines: lifting the ban on total dietary fat. J Am Med Assoc 2015; 313: 2421-2422.
- Mozaffarian D: Foods, nutrients, and health: when will our policies catch up with nutrition science? Lancet Diabetes Endocrinology 2016; 5(2): 85-88.
- Dehghan M, et al: Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet 2017; 390(10107): 2050-2062.
- Gastromed Suisse: Nutrition. Health: How harmful is sugar, 2015. www.gastromed-suisse.ch
- Barazzoni R, et al: Carbohydrates and insulin resistance in clinical nutrition: recommendations from the ESPEN expert group. Clin Nutr 2017; 36: 355-363.
- Seneff S, et al: Is the metabolic syndrome caused by a high fructose, and relatively low fat, low cholesterol diet? Arch Med Sci 2011; 1: 8-20.
- de Lorgeril M, et al: Mediterranean diet, traditional risk factors and the rate of cardiovascular complications after myocardial infarction. Final Report of the Lyon Diet Heart Study. Circulation 1999; 99: 779-785.
- Vormund K, et al: Mediterranean diet and mortality in Switzerland: an alpine paradox? Eur J Nutr 2015; 54(1): 139-148.
CARDIOVASC 2018; 17(2): 26-30