
Patients with soft tissue sarcoma often complain of localized pressure and increasing pain. In addition to sonography, contrast-enhanced CT and MRI imaging are particularly informative. If there is a suspicion of a malignant soft tissue tumor based on the imaging findings, a histological clarification by means of a biopsy is indicated. Nowadays, a fine needle biopsy is often sufficient for this.
Soft tissue sarcomas can occur anywhere in the human body. About 60% occur on the extremities. They represent a heterogeneous entity of rare malignancies that can be localized intra- or retroperitoneally in the abdominal cavity. They often grow slowly, so that the symptoms only become evident in the late stages when the tumor is considerably larger [1,2,9]. In addition to organ displacement, infiltrative growth is also possible. Occasionally several organs are involved. The most common sarcoma is liposarcoma [8] with a proportion of around 20%, followed by malignant schwannoma, leiomyosarcoma and malignant fibrous histiocytoma [5]. Low-grade tumors and macroscopically tumor-free surgical sites are significantly associated with a reduced risk of recurrence and improved prognostic survival.
Metastasis is usually hematogenous. In about 70% of cases, the filiae metastasize to the lungs and liver, including the peritoneum. The biological behavior of these masses depends on the histology, the degree of differentiation, the site of manifestation in the body and the age of the patient. The response to the measures accompanying surgical treatment varies greatly, as shown in Table 1 .
The incidence of retroperitoneal sarcomas is 1-3/100,000 per year, with a mortality rate of 0.6 to 0.8/100,000 per year [4]. The symptoms are characterized by swelling or circumferential enlargement, abdominal or lumbar pain, paresthesia of the lower extremities or digestive disorders. Approximately 20% of patients present with B symptoms.
Advances in the diagnosis of the tissue and genetic structure of soft tissue malignancies are increasingly allowing a more precise characterization of sarcomas. The material from the fine needle biopsy is often sufficient to cytologically classify the sarcomatous process [10]. The combination of surgery, radiotherapy and chemotherapy for sarcomatous soft tissue processes has significantly improved the 3-year survival rate from 20 to 75% in recent years. For radiotherapy in particular, this has meant more precise planning and optimal fractionation and tumor dose in order to reduce the rate of radiotherapy-related side effects [3].
Small tumors that have been present for a long time and are reliably localized subcutaneously by clinical examination can be detected sonographically and their echogenicity, contour and size can be assessed [2]. They can then be sent for excisional biopsy. Soft tissue sarcomas are almost exclusively hypervascularized, predominantly homogeneously low-echo, rarely also homogeneously high-echo [6,7]. Sonography is a suitable imaging tool for the rapid clarification of lymph node and liver metastases.
The different tissue components of sarcomas can be differentiated and quantified very well using computer tomography. Fatty tissue masses are malignant if they contain connective tissue or thicker septa. Calcifications can be differentiated in about 12% of malignancies [8].
The sarcomas show a variable signal on magnetic resonance imaging. The liposarcomas are dominated by hypointense signals in fat-suppressing sequences [8]. The contrast agent reactions are highly variable. Fatty tissue conglomerates over 6 cm are tumor-suspect, especially with heterogeneous tissue structure.
Case study
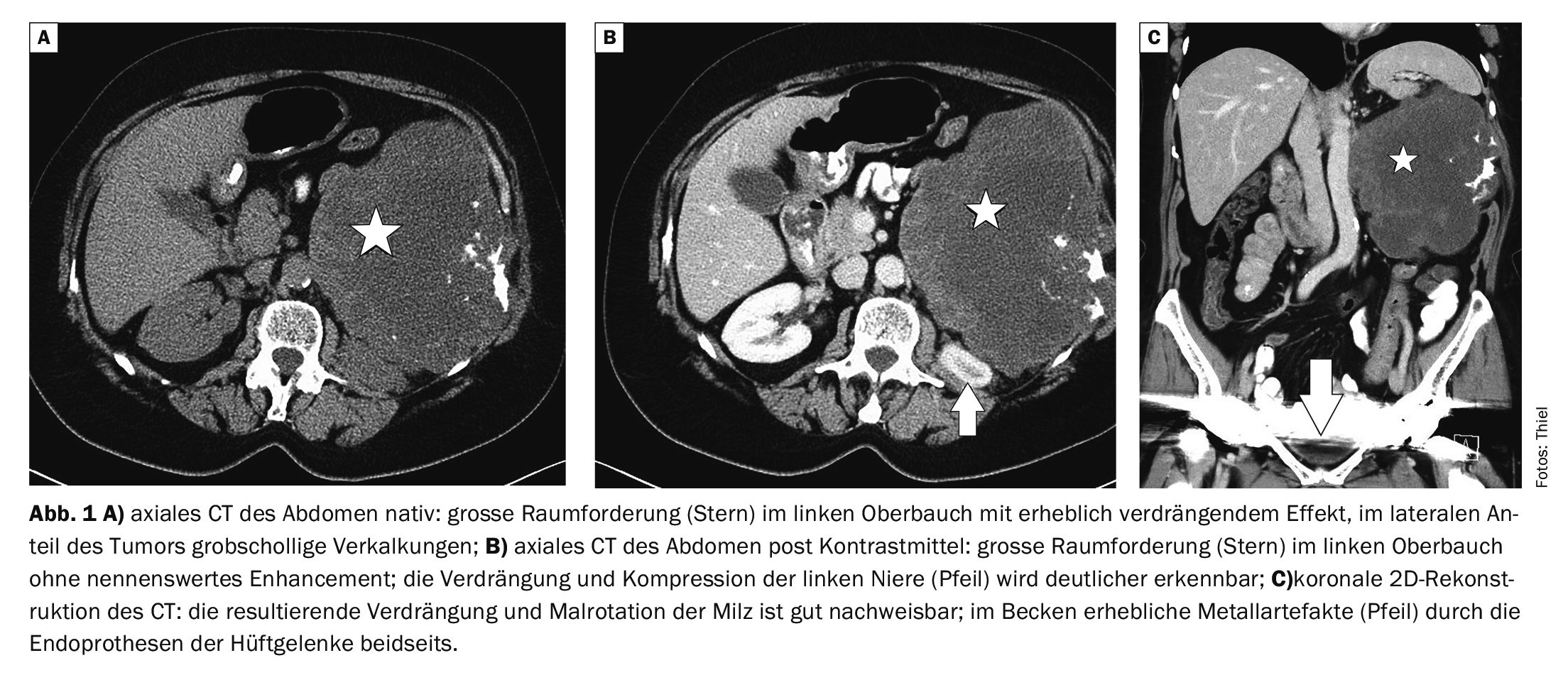
In case example 1 (Fig. 1A to 1C) , a 62-year-old female patient was referred from the urology outpatient clinic with a suspected left renal tumor. Computed tomography showed a large mass measuring 16 × 16 × 14 cm, which had a considerable local organ-displacing effect. The contour was relatively smooth, the internal structure inhomogeneous with coarse calcifications. The patient complained of a feeling of pressure in the upper abdomen and progressive pain. The findings were surgically removed. Histologically, a chondromyxoid sarcoma was found.
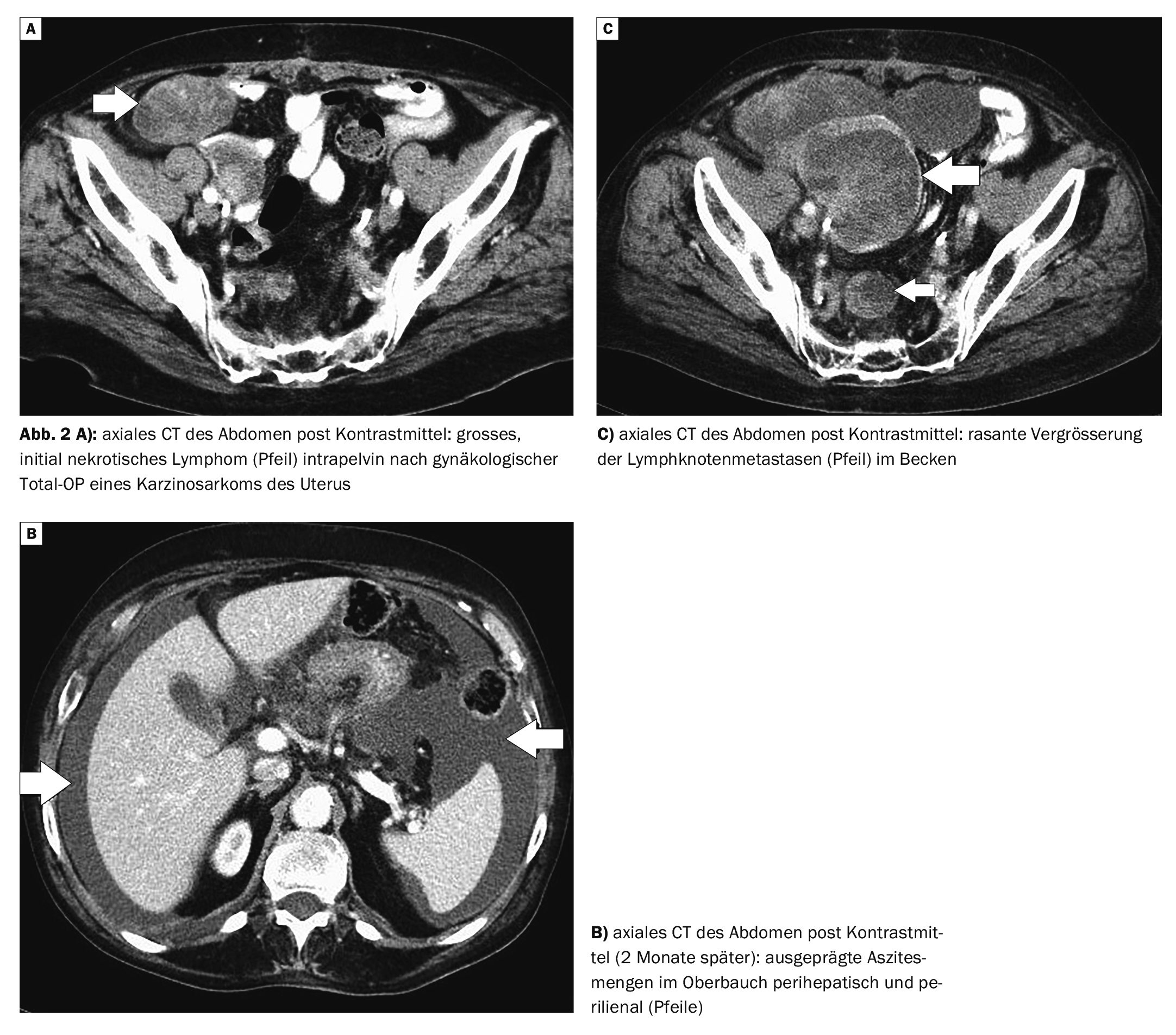
Case 2 demonstrates (Fig. 2A to C) the course of a carcinosarcoma of the uterus in an 82-year-old female patient following primary surgery. About four months postoperatively, increasing lower abdominal pain and weight loss developed. Computed tomography control showed intrapelvic lymph node and peritoneal metastases, which led to numerical and size progression and ascites at a further control 2 months later. To ensure urinary drainage, both ureters were fitted with DJ splints. Pulmonary metastasis was also detected.
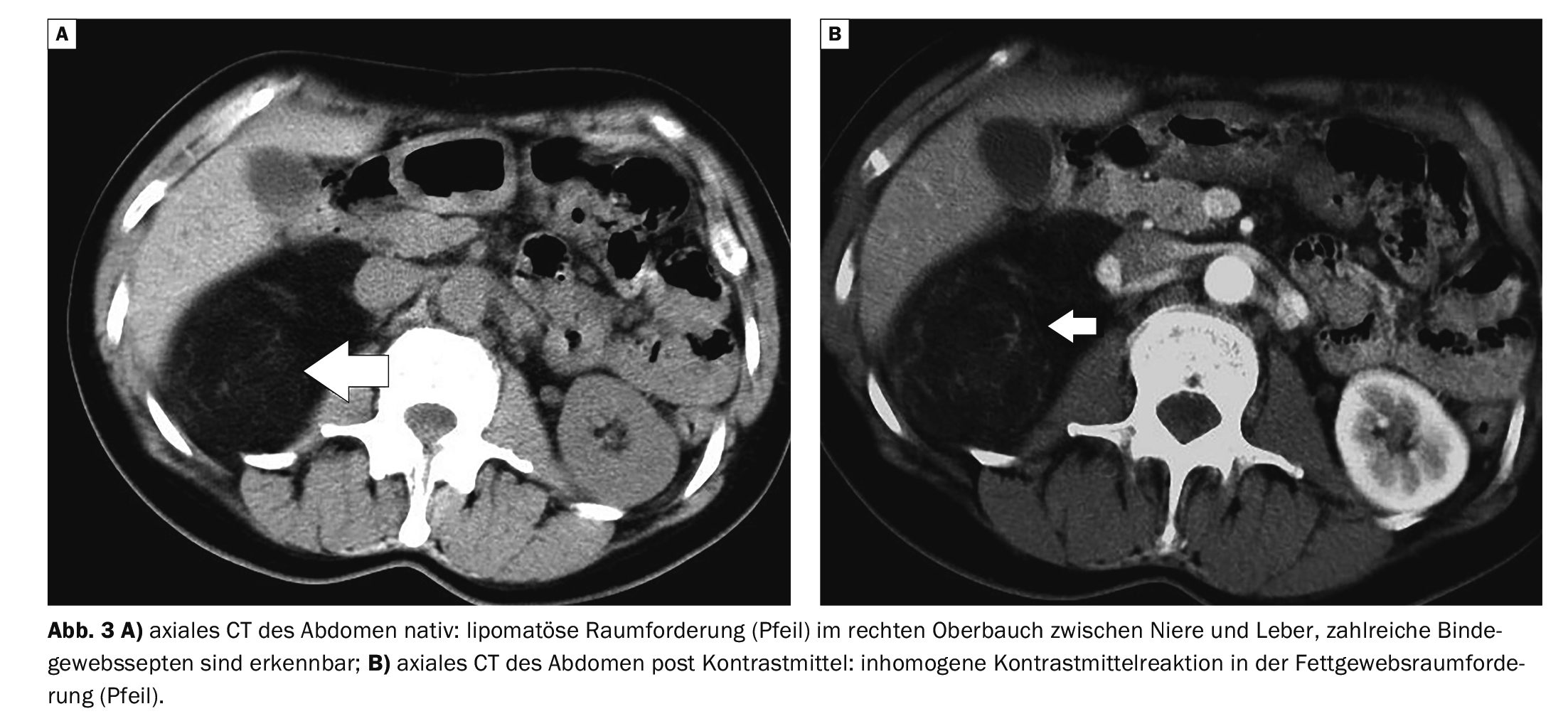
Case 3 shows a 56-year-old female patient with a liposarcoma at the upper right renal pole with contact to the liver (Fig. 3A and B). The finding was noticed during a routine abdominal sonography by the family doctor, but there were no symptoms. Computed tomography confirmed the suspicion of a 6 cm liposarcoma, and the tumor entity was confirmed surgically and histologically.
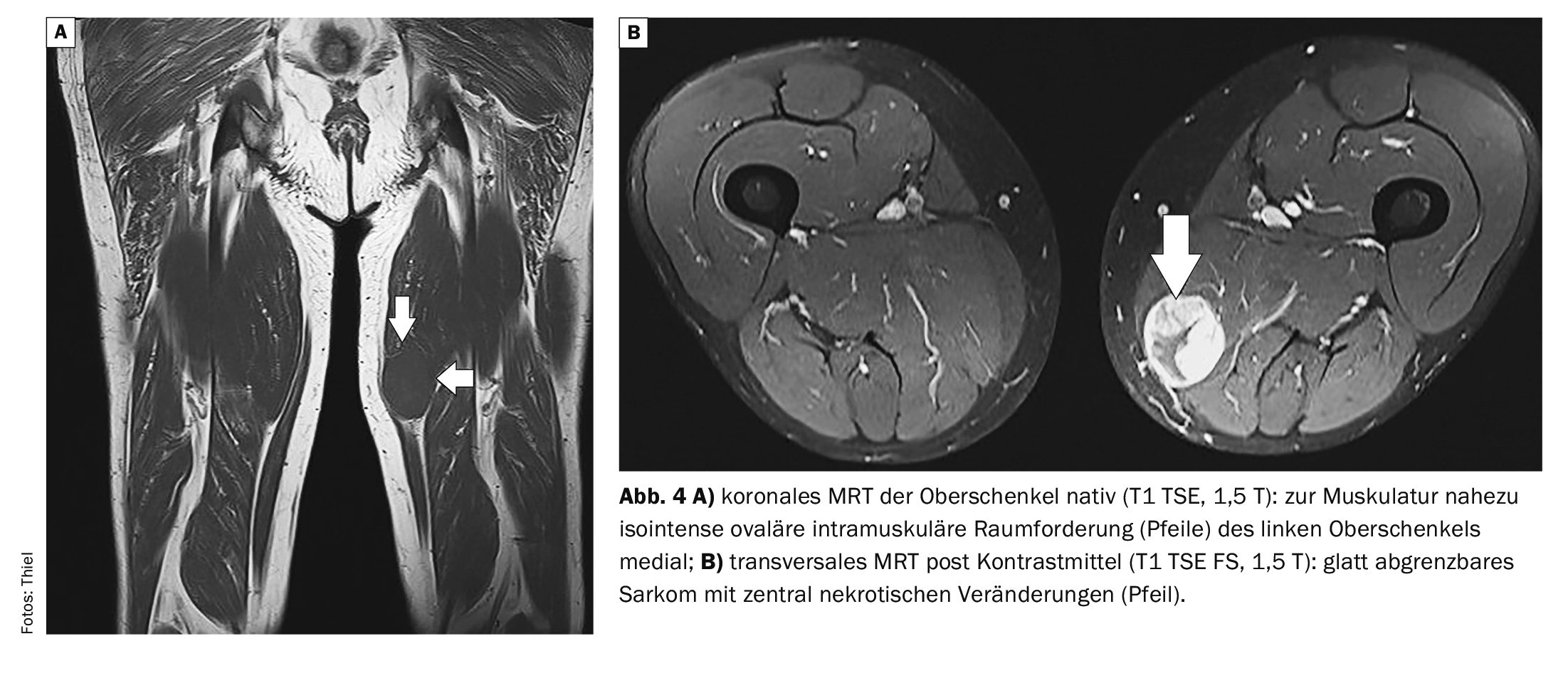
In case 4 (for comparison), an intramuscular tumor was detected on MRI of the left thigh in a 67-year-old patient (Fig. 4A and B). Clinically, a relatively coarse and rapidly growing, indolent tumor was found. The mass was clearly demarcated in the section. Surgical extirpation revealed a biphasic epithelial sarcoma. Postoperative radiotherapy was performed.
Take-Home-Messages
- Sarcomas are rare malignant tumors.
- A distinction is made between different histological types. Liposarcomas make up the largest proportion of these.
- Middle-aged and older adults are primarily affected.
- Computed tomography and magnetic resonance imaging are the best imaging techniques for showing the overall extent of tumors and their relationship to other organs.
- The treatment of choice is radical surgery, supplemented by radiotherapy and chemotherapy.
Literature:
- Alldinger I, Alexander A, Knoefel WT: Soft tissue sarcomas of the retroperitoneum. General and Visceral Surgery up2date 2010; 4(1): 19-34.
- Bannasch H, et al: Diagnosis and therapy of soft tissue sarcomas of the extremities. Dtsch Arztebl Int 2011; 108(3): 32-38.
- Golubicic I, et al: Role of radiotherapy in combined therapy of soft tissue sarcoma in children and adolescents. Srp Arh Celok Lek 2000; 128(5-6): 172-178.
- Manski D: Urologielehrbuch.de; www.urologielehrbuch.de/
retroperitoneales_sarkom.html, (last accessed 10.09.2024). - Mofid H, et al: Retroperitoneal sarcomas in adulthood. Visceral Surgery 2001; 36(4): 222-228.
- Reichardt P: Diagnosis of soft tissue tumor. www.krebsgesellschaft.de,(last accessed 10.09.2024).
- Schulte M, et al: Sonographic classification of solid soft tissue tumors. TumorDiagnostics & Therapy 2010; 31(4): 215-223.
- Thiel HJ: Cross-sectional imaging of the spine 7.32. Incidental findings: retroperitoneal liposarcoma. MTA Dialog 2017; 18 (1): 13-17.
- Visceral and retroperitoneal sarcomas, www.uniklinikum-leipzig.de/einrichtungen/vttg/Seiten/sarkome.aspx,(last accessed 10.09.2024).
- Wakely Jr PE: Extraskeletal myxoid chondrosarcoma: combining cytopathology with molecular testing to achieve diagnostic accuracy. J Am Soc Cytopathol. 2021;10(3): 293-299.
FAMILY PHYSICIAN PRACTICE 2024; 19(10): 49-52









