
Childhood leukemias are treated in a risk-adapted manner and are curable in the majority of cases. In acute lymphoblastic leukemia, one of the most important prognostic factors – in addition to classical prognostic markers such as leukemic subtype and cytogenetic changes of leukemic blasts – is the determination of minimal residual disease after therapy induction. Current developments aim at a more effective treatment of previously resistant leukemia subtypes as well as a reduction of therapy toxicity.
Leukemias are the most common childhood and adolescent cancers in industrialized countries, accounting for approximately 35% of all neoplasms. In Switzerland, we diagnose 55-65 new cases annually. The current incidence in children under 15 years of age is approximately 4.9 cases/100,000 population. The two major forms of childhood leukemia are acute lymphoblastic leukemia (ALL) (approximately 82%) and acute myeloid leukemia (AML) (approximately 15%). Only rarely do myelodysplastic syndromes and chronic myeloid leukemias occur in children.
Acute lymphoblastic leukemia
The most common childhood ALL is B-precursor ALL, which develops from immature cells of the B-series of the lymphatic system. More rarely, ALL of the T lymphopoiesis occurs. A special form is mature B-cell leukemia, which is due to malignant transformation of the mature B-cell and is understood as a leukemic manifestation of Burkitt’s lymphoma. The cause of leukemia development remains unclear and continues to be the focus of many epidemiological studies. Known but rarely occurring factors are ionizing radiation and congenital syndromes. However, this explains less than 10% of all diseases. It is estimated that approximately 1% of children born with Down syndrome develop leukemia (ALL or AML) within the first five years. Their risk is increased about 20 times compared to healthy children. Even more frequently (in 3-10%), however, transient myeloproliferation occurs in the neonatal period in these children, which occasionally may later progress to leukemia. Other rarer congenital changes with increased risk of leukemia include ataxia teleangiectatica, Fanconi syndrome, and other syndromes associated with immunodeficiency or increased chromosomal fragility.
Various observations have led to different hypotheses regarding an infection-associated leukemia development: e.g. the facts that ALL occurs more frequently between the second and fifth year of life, that a clustering of the disease can be seen in industrialized countries, or that in the past clustering has repeatedly occurred especially in regions of new agglomerations. [1,2].
Symptoms of ALL
In the foreground are symptoms due to the displacement of normal blood cell formation in the bone marrow, such as pallor and fatigue due to anemia or bleeding tendencies due to thrombocytopenias. Infiltration leads to diffuse bone pain and alternating arthropathies, which occasionally manifest themselves in young children as reluctance to move or even refusal to walk. Furthermore, lymph node swelling as well as organomegaly may occur.
Diagnostics of ALL
In the blood, changes in at least two blood cell series are often found, most commonly thrombocytopenia with concomitant anemia. The leukocyte count may be normal, decreased or increased. The morphology of the blood count can provide important diagnostic clues, and the final diagnosis is made by bone marrow aspiration. Hereby, in addition to the examination of the morphology, the immunophenotype of the leukemic blasts is determined by flow cytometry (FACS) and a chromosome analysis is performed. Immunophenotyping allows to determine the developmental stage of the corresponding cell clone.
The most common leukemia subtype in children, so-called “common-ALL”, is characterized by expression of the B-cell markers CD10 and CD 19. Expression of myeloid antigens, usually however not prognostically significant, can be detected in almost half of ALL.
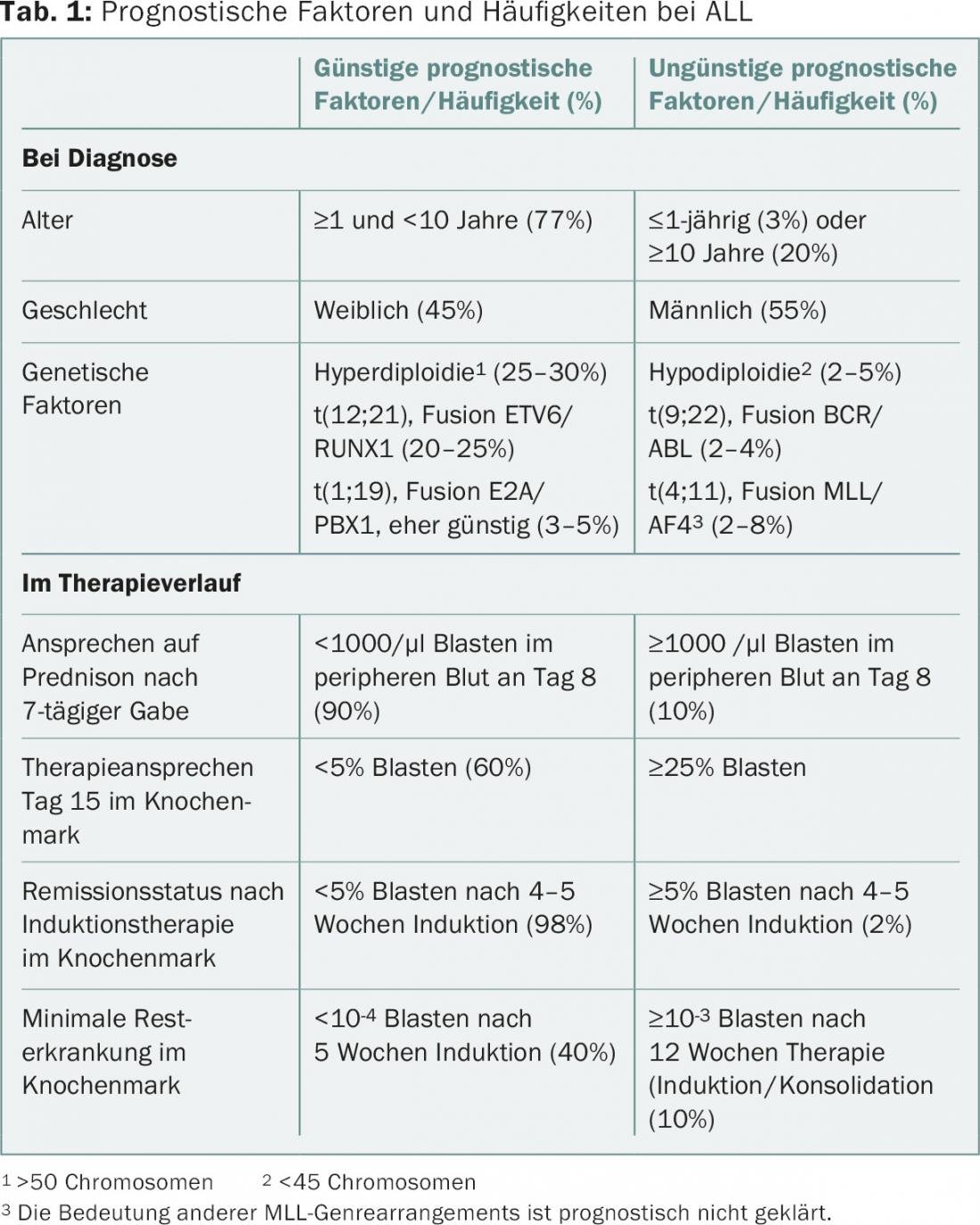
Today, cytogenetic and molecular genetic diagnostics play an important role. It is important to identify the most important subgroups, as they have therapeutic implications. On the one hand, numerical chromosome alterations such as hyper- or hypodiploidy as well as structural alterations such as translocations, e.g. t(12;21) (fusion of ETV6/RUNX1 genes) or t(9;22) (fusion of BCR/ABL1), MLL rearrangements (MLL 11q23) and other alterations are sought. Classically, these alterations are detected by conventional cytogenetics (G-banding) and/or fluorescent in situ hybridization (FISH) in the leukemia cells. The most common chromosomal alterations in ALL are shown in Table 1 .
Treatment response is a very important prognostic parameter. In recent years, the measurement of minimal residual disease (MRD) from bone marrow has become established in the context of follow-up diagnostics for the assessment of therapy response. Two main methods are used, which complement each other in clinical practice. The most sensitive method is monitoring immunoglobulin and T-cell receptor rearrangements. This involves an initial search for leukemia-specific clonal rearrangements, which are followed by quantitative PCR at specific therapy time points. The detection limit thus achieved is approximately one leukemia cell per 100,000 normal bone marrow cells. A technique of MRD measurement that is less sensitive by approximately one log level is based on monitoring of the leukemia-associated immunophenotype by FACS. A sensitivity of 0.001% can be achieved [3].
Therapy and prognosis of ALL
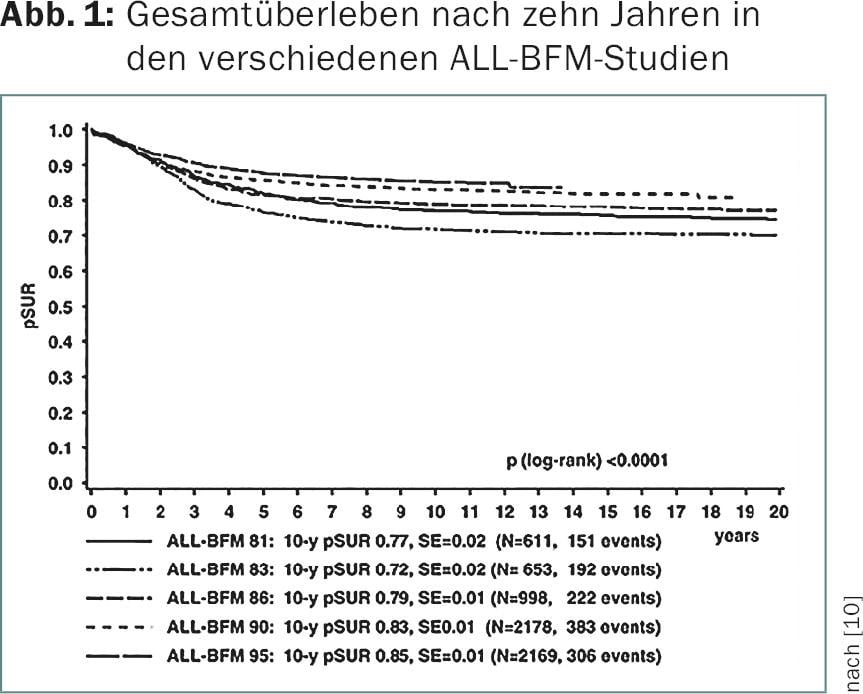
Continued adaptation of treatment for ALL over the past 40 years has led to a dramatic increase in survival. The ALL-BFM Study Group, a consortium of German, Austrian and Swiss pediatric oncology centers, has contributed significantly to this improvement in numerous large-scale randomized therapy trials since 1976.
Induction therapy should achieve remission and restoration of normal hematopoiesis within the first four to six weeks of therapy. This is possible with current modalities in approximately 98% of all patients with the three drugs cortisone, vincristine, and asparaginase; in some study groups, patients also receive an anthracycline [4–6]. In the ALL-BFM protocols we use, remission induction is initiated by seven days of monotherapy with prednisone and intrathecal administration of methotrexate. In the majority of cases, complications due to cell decay can be avoided, and an initial assessment of the sensitivity of the leukemia cells to these drugs can already be investigated (prednisone response). Particularly CNS-impacting consolidation (high-dose methotrexate) is followed by re-induction therapy; it has been shown that repeated use of induction therapy after a period of consolidation can substantially reduce the risk of recurrence [5,7]. Equally indispensable components of successful leukemia treatment are extracompartmental therapy (CNS preventive treatment) and prolonged continuous maintenance therapy, which provides remission by suppressing resistant leukemia clones. Nowadays, the prevention of CNS recurrence is mostly done by drugs, on the one hand by intrathecal methotrexate injections, on the other hand by systemically acting cytostatic drugs infiltrating the brain (e.g. high-dose methotrexate). As a result, earlier radiotherapy of the CNS could be limited to very special risk situations; although this leads to a dramatic reduction in CNS recurrences, it is associated with not inconsiderable late effects [4,5,8].
Of particular relevance nowadays are risk-adapted therapy strategies, which result from various biological parameters such as cytogenetics and initial therapy response (Tab. 1). On the one hand, the aim is to improve the prognosis in high-risk leukemias by further intensification of therapy or selective use of new substances; on the other hand, the aim is to avoid unnecessary toxicity with a favorable prognosis. Cell number, age, sex, cytogenetics, and initial peripheral blood lymphoblast response to prednisone administration within the first eight days are factors that influence prognosis [9]. Further response in the context of therapy induction is also a prognostically relevant parameter.
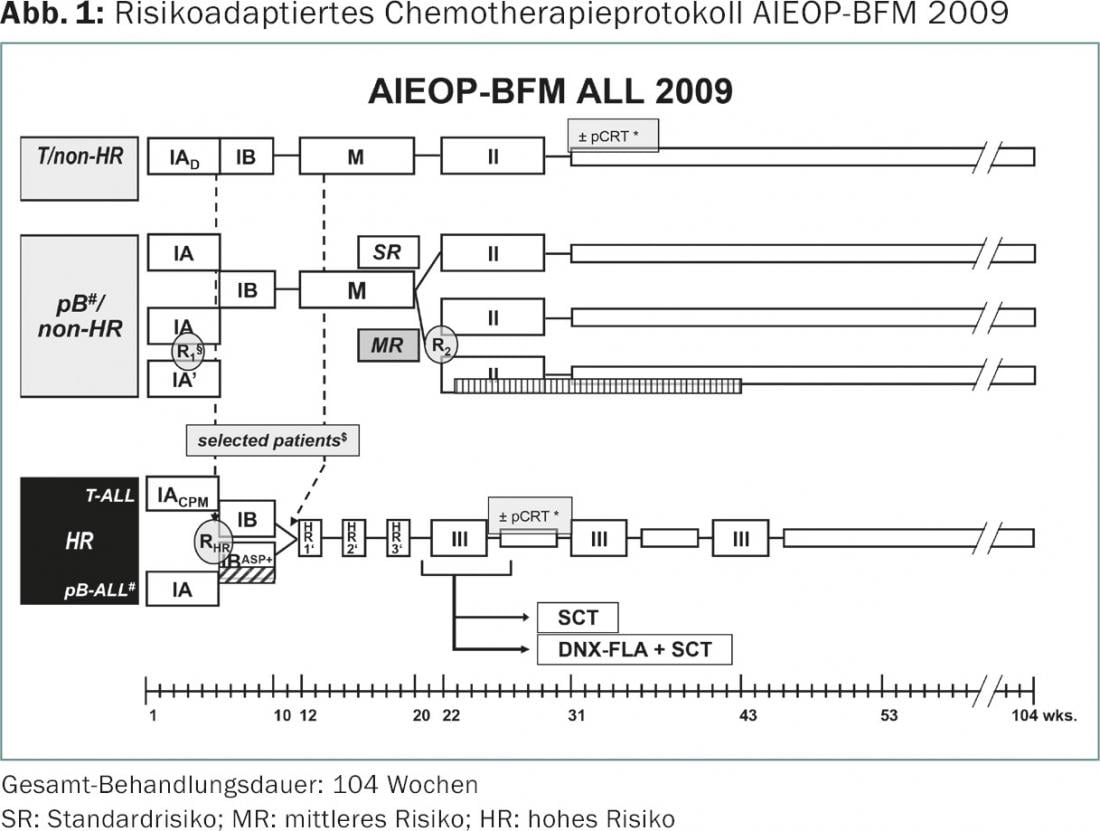
Therapy study AIEOP-BFM ALL 2009
Most centers in Switzerland treat children with ALL in the multicenter therapy study AIEOP-BFM ALL 2009. In addition to the “old” BFM countries Switzerland, Germany and Austria, four other countries (Italy, Israel, Australia, Czech Republic) have agreed on a common treatment protocol (Fig. 1) . The aim of the study is to jointly enroll about 4000 children and adolescents with ALL and to randomly test several therapy-relevant questions. Assignment to the three risk groups SR (standard risk), MR (intermediate risk) and HR (high risk) is based on biological criteria such as hypodiploidy or MLL rearrangement on the one hand, and on the assessment of treatment response using the various MRD techniques on the other. Factors included in risk stratification are: leukemia response to the 7-day steroid pre-phase, the decline in leukemia cells in the bone marrow measured by FACS on therapy day 15, and minimal residual disease on days 33 and 78 after initiation of therapy as measured by the decline in leukemia-specific immune and T-cell receptor rearrangements by quantitative PCR [10].
In children with a very good response to the first 15 days of therapy as measured by FACS-MRD, a reduction in anthracycline doses during the induction phase to two instead of four doses will be tested (R1). For the largest patient group MR, the benefit – in terms of recurrence risk – of nine additional administrations of long-acting pegylated asparaginase over the duration of 20 weeks at the end of the intensive chemotherapy phase will be randomly tested (R2). The third randomization is for HR patients who, despite intensive efforts in recent decades, still achieve only about 50% freedom from recurrence. In this group of patients, therapy should be intensified with four additional asparaginase administrations already in the induction phase (RHR).
Treatment for recurrence
The outcomes of primary therapy as well as relapse protocols for leukemias have improved over time. With current risk-adapted therapies, long-term survival rates of approximately 85% are achieved (Fig. 2) [7]. This also led to a continuous adjustment of the indication for high-dose therapies with stem cell reinfusion. An international stem cell transplantation protocol (ALL-SCT-BFM 2003) has attempted to establish clear definitions for the indication of allogeneic stem cell transplantation, both in the setting of primary therapy and in relapses. Currently, there is an indication for bone marrow transplantation as part of primary therapy for certain prognostically unfavorable cytogenetic subgroups, such as t(9;22), or for insufficient response to therapy in induction therapy [11].
From the experience of the BFM group, it has been shown that treatment success in relapses depends on the time of relapse occurrence, the pattern of leukemia attack, and the leukemia subtype [12]. The therapy response after renewed therapy induction and thus the dynamics of the decline in minimal residual disease is also of particular prognostic importance here; accordingly, further therapy elements, such as bone marrow transplantation, are aligned accordingly [13]. There is reasonable hope that targeted therapy with antibodies or more specific kinase inhibitors will be possible in the future for various subtypes of ALL. As an example, the CD19 antibody (blinatumomab) was able to induce encouraging remission rates in phase I and II trials in relapsed ALL [14]. Other potential therapeutic approaches of targeted therapies involve interactions with signaling pathways within leukemia cells. These include, for example, suppression of CRLF2 gene expression or abnormal JAK gene activation.
Acute myeloid leukemia
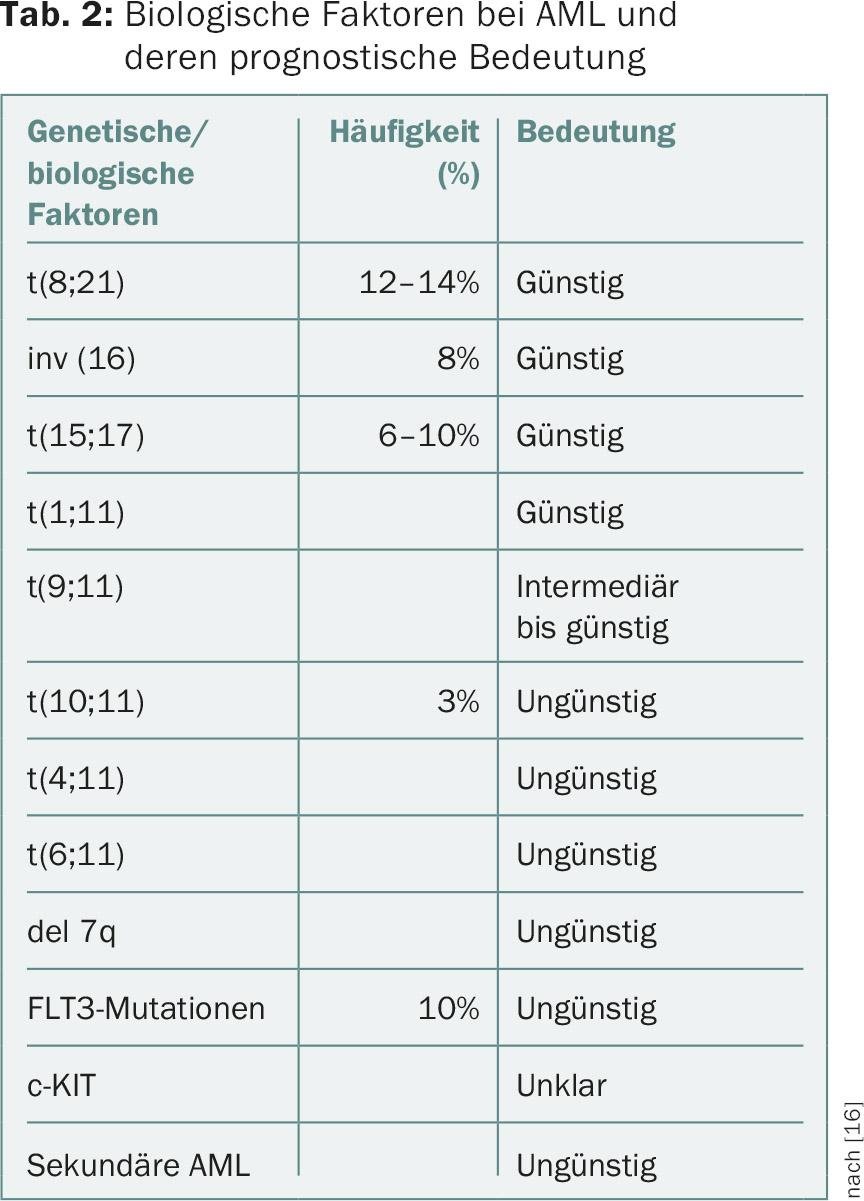
AML involves a myeloid stem or progenitor cell responsible for the formation of granulocytes, monocytes, platelets or erythrocytes. In AML, in contrast to ALL, immunologic subtyping is of less importance. Also in AML, in addition to the morphologic subtype (M0-M7 according to FAB classification), genetic factors as well as response to therapy and monitoring of residual disease are important parameters in prognostic evaluation [15]. Translocations such as t(8;21) especially in AML, FAB M1/M2, t(15;17) typical in AML, FAB M3, inversion(16) in AML and FAB M4 Eo are favorable factors, whereas certain subtypes with MLL rearrangement (11q23) or FLT3 gene mutation are prognostically unfavorable (Table 2) [16].
There also does not appear to be a one-size-fits-all therapy for all subgroups in AML. While in acute promyelocytic leukemia (AML, FAB M3) the introduction of retinoic acid significantly reduced the complication rate and improved the cure rate, other subtypes are almost impossible to manage without bone marrow transplantation. Hyperleukocytosis in AML as well as FAB M3 subtype is an emergency situation and requires rapid intervention as the risk of bleeding is significantly increased.
The critical drugs for remission induction in AML are cytarabine and anthracyclines [17,18]. Etoposide is often added as well. The additional benefit of postinduction chemotherapy, again with high-dose cytarabine, has been demonstrated several times. In recent years, additional 2-CDA (2-chloro-2-deoxyadenosine) has been successfully used in high-risk leukemias, especially in combination with cytarabine. This combination leads to maximum inhibition of DNA synthesis. In contrast to ALL, the use of maintenance therapy is still controversial in AML [19]. The approach to CNS-directed therapy is also inconsistent. It ranges from intrathecal monotherapy with cytarabine or methotrexate to triple therapy with cytarabine, methotrexate, and hydrocortisone, with or without additional radiotherapy. In general, however, radiotherapy has been significantly reduced or even eliminated in AML in recent years.
The cure rate in AML is highly dependent on the above parameters, but today reaches up to 70%. Allogeneic stem cell transplantation is still generously recommended in certain study groups when a compatible sibling donor is available. Others prefer a risk-adapted indication for stem cell transplantation (SCT). In general, however, there is an increased reluctance to recommend SCT. In any case, SCT is indicated in cases of incomplete remission or recurrence. Hope is pinned on the targeted use of kinase inhibitors for detected mutations, such as FLT3 or KIT mutations.
Late effects of leukemia treatments
As survival rates after leukemias increase, attention to late effects naturally increases. For example, long-term cardiotoxicity after therapy for AML must be considered. Osteonecrosis and other vascular events, which are common in ALL, may also cause long-term morbidities. After SCT, late effects are more frequent and relevant. The risk of secondary malignancies again depends on the cytostatic drugs used, and an increased risk also exists after radiotherapy.
Literature:
- Kinlen L: Infections and immune factors in cancer: the role of epidemiology. Oncogene 2004; 23: 60-75.
- Greaves M: Infection, immune responses and the aetiology of childhood leukaemia. Nat Rev Cancer 2006; 6(3): 193-203.
- Campano D: Minimal residual disease monitoring in childhood acute lymphoblastic leukemia. Curr Opin Hematol 2012; 19: 313-318.
- Pui CH, Evans WE: Treatment of childhood acute lymphoblastic leukemia. N Engl J Med 2006; 354: 166-178.
- Möricke A, et al: Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 95. Blood 2008; 111(9): 4477-4489.
- Schrappe M, et al: Long-term results of four consecutive trials in childhood ALL performed by the ALL-BFM study group from 1981 to 1995. Berlin-Frankfurt-Münster. Leukemia 2000; 14(12): 2205-2222.
- Möricke A, et al: Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981 to 2000. Leukemia 2010; 24(2): 265-284.
- Kamps WA, et al: BFM-oriented treatment for children with acute lymphoblastic leukemia without cranial irradiation and treatment reduction for standard risk patients: results of DCLSG protocol ALL-8 (1991-1996). Leukemia 2002; 16(6): 1099-1111.
- Schrappe M, et al: Improved outcome in childhood acute lymphoblastic leukemia despite reduced use of anthracyclines and cranial radiotherapy: results of trial ALL-BFM 90. German-Austrian-Swiss ALL-BFM Study Group. Blood 2000; 95(11): 3310-3322.
- International Collaborative Treatment Protocol For Children And Adolescents With Acute Lymphoblastic Leukemia. http://clinicaltrials.gov/show/NCT01117441.
- Balduzzi A, et al: Chemotherapy versus allogeneic transplantation for very-high-risk childhood acute lymphoblastic leukaemia in first complete remission: comparison by genetic randomisation in an international prospective study. Lancet 2005; 366: 635-642.
- Tallen G, et al: Long-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: results of trial ALL-REZ BFM 90. J ClinOncol 2010; 28: 2339-2347.
- Eckert C, et al: Minimal residual disease after induction is the strongest predictor of prognosis in intermediate risk relapsed acute lymphoblastic leukaemia – Long-term results of trial ALL-REZ BFM P95/96. Eur J Cancer 2012; http://dx.doi.org/10.1016/j.ejca.2012.11.010.
- Schlegel P, et al: Pediatric posttransplant relapsed/refractory B-precursor acute lymphoblastic leukemia shows durable remission by therapy with the T-cell engaging bispecific antibody blinatumomab. Haematologica 2014; 99(7); 1212-1219.
- Abrahamsson J, et al: Response-guided induction therapy in pediatric acute myeloid leukemia with excellent remission rate. J ClinOncol 2011; 29(3): 310-315.
- Creutzig U, et al: AML Committee of the International BFM Study Group. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood 2012; 120(16): 3187-3205.
- Creutzig U, et al: Treatment strategies and long-term results in paediatric patients treated in four consecutive AML-BFM trials. Leukemia 2005; 19(12): 2030-2042.
- Creutzig U, et al: Less toxicity by optimizing chemotherapy, but not by addition of granulocyte colony-stimulating factor in children and adolescents with acute myeloid leukemia: results of AML-BFM 98. J ClinOncol 2006; 24(27): 4499-4506.
- Perel Y, et al: Group LAME of the French Society of PediatricHematology and Immunology. Impact of addition of maintenance therapy to intensive induction and consolidation chemotherapy for childhood acute myeloblasticleukemia: results of a prospective randomized trial, LAME 89/91. J Clin Oncol 2002; 20(12): 2774-2782.
InFo ONCOLOGY & HEMATOLOGY 2015; 14(5): 8-12.









