Levodopa treatment in Prakinson’s disease often results in motor fluctuations and dyskinesias. For selected patients in advanced stages, deep brain stimulation, which works by applying high-frequency pulses to specific brain areas, has proven to be the gold standard. In particular, fluctuations can be well treated by this, but also non-motor symptoms such as levodopa-responsive pain. Overall, deep brain stimulation, which is only offered by a few centers in Switzerland within the framework of highly specialized medicine, should be considered in patients with PD who cannot be treated sufficiently well with drug therapy methods, i.e., in whom motor symptoms or quality of life cannot be satisfactorily improved by oral therapies. The indication must be checked as soon as the first fluctuations in effect occur, as the risk-reward ratio deteriorates as the disease progresses.
Along with Alzheimer’s disease, Parkinson’s disease (or: idiopathic Parkinson’s syndrome) is one of the most common neurodegenerative diseases, with demographic trends and the associated fact that people are getting older contributing significantly to the fact that the prevalence continues to increase. PD manifests not only with motor symptoms, but also with a variety of non-motor symptoms.
Treatment of the classic motor symptoms of bradykinesia, rigor, and tremor is based primarily on replacement of substances that target striatal dopamine receptors, leading to partial reconstitution of normal basal ganglia function. At the beginning of therapy, this strategy leads to very good control of symptoms in most PD patients, although tremor, if present, does not respond to dopaminergic drugs in all patients. In the longer term, treatment with dopaminergic substances, but especially with levodopa preparations, often leads to motor fluctuations and dyskinesias. This leads to a deterioration in the independence and quality of life of those affected.
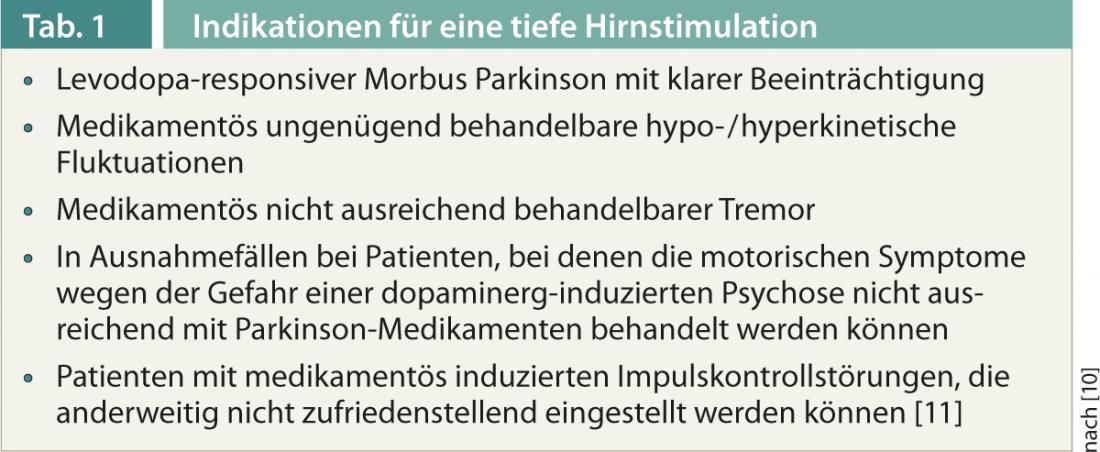
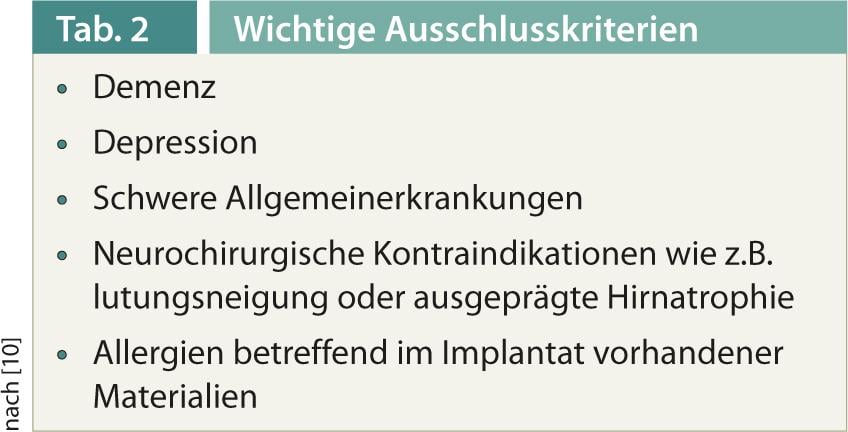
Today, there are several possible treatment escalations for these advanced-stage patients, and deep brain stimulation is now established as an excellent evidence-based gold standard for carefully selected patients (Tables 1 and 2).
As early as 1987, high-frequency electrical modulation of neuronal activity in the nucleus subthalamicus was shown to lead to reversible improvement of Parkinson’s symptoms, which was confirmed in initial clinical studies [1–3]. In the meantime, large randomized trials are available that have tested the efficacy of deep brain stimulation versus best drug treatment [4, 5]. The efficacy is therefore clearly proven, and so is the positive influence on the quality of life, which explains why over 100,000 patients have been treated with this method worldwide to date.
Functionality and effect
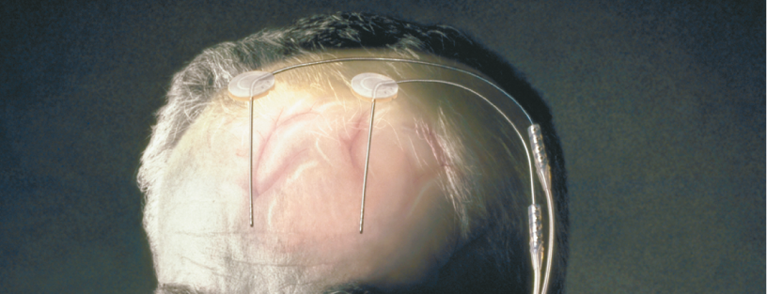
Deep brain stimulation works by applying high-frequency pulses in defined brain areas, with electrodes connected to the actual stimulator (“brain pacemaker”) by means of subcutaneous cables and modulating the function of neurons, their connections and thus signal transmission in the basal ganglia in the corresponding central nervous target area (Fig. 1).
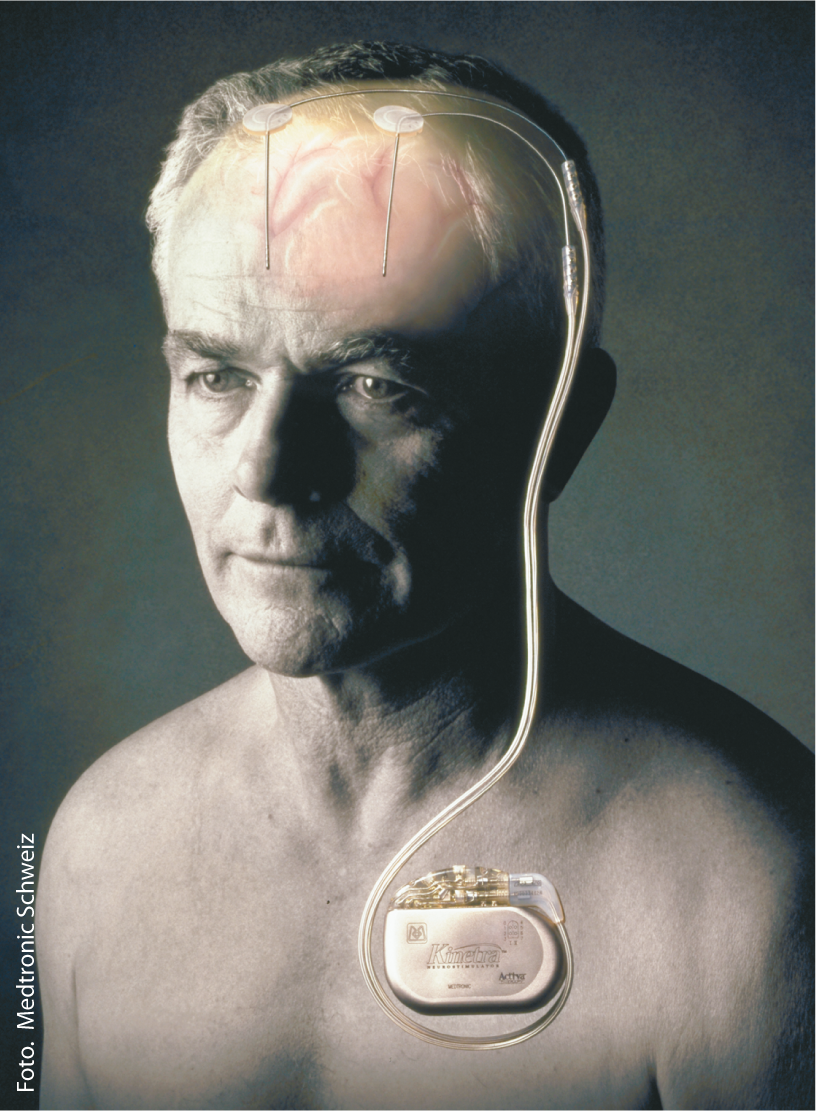
Fig. 1: Electrodes and stimulator
The therapy improves both motor symptoms and especially fluctuations: Patients are in a good motor state longer and are less hypo- or dyskinetic [4, 5]. In principle, the better rigor and bradykinesia respond to levodopa, the higher the efficacy of stimulation. Tremor also responds, in this case also in the absence of response to dopaminergic drugs. Axial symptoms such as postural instability or postural dysfunction, on the other hand, do not respond to medication or deep brain stimulation. The effect lasts for years, with partial decay possible under stimulation in the globus pallidus. With subthalamic stimulation, medications can be reduced postoperatively.
On non-motor symptoms, deep brain stimulation also has therapeutic effects, especially on levodopa-responsive pain, which can remit under subthalamic stimulation [6]. Possibly due to co-stimulation of the limbic parts of the nucleus subthalamicus, there may be an elevation of mood, up to a hypomanic state.
Reducing the daily drug dose in subthalamic stimulated patients may reduce drug-induced side effects, particularly impulse control disorders or excessive daytime sleepiness. In contrast, too rapid a reduction in dopaminergic medication can lead to apathy and depression.
Side effects and complications
Side effects such as gait disturbances, dysarthria, hypomania, oculomotor disturbances or dyskinesia can occur depending on the stimulation site and intensity and can be minimized on the one hand by testing in the operating room on the awake patient and on the other hand by adjusting the stimulation in the first weeks to months after surgery, but cannot always be avoided. Device-specific complications such as cable breakage or dyslocations occur sporadically, but especially after trauma.
The surgical risks are small, but intracranial hemorrhage and infection cannot be completely ruled out even with the best possible preparation and execution. The battery life is 2-7 years depending on the intensity of stimulation, the battery change itself is uncomplicated.
Which target point in the brain?
The subject of discussion is which target in the brain is the most effective and best tolerated for Parkinson’s patients. Both the nucleus subthalamicus and globus pallidus internus are regularly used as targets, with most experts interpreting the nucleus subthalamicus as the more effective target structure, although this debate cannot be considered closed [7, 8]. On the other hand, stimulation in the globus pallidus has advantages with regard to neuropsychiatric tolerance, which is why the optimal procedure must be decided separately for individual patients. Other possible target areas are currently being discussed in the literature, but cannot be addressed in this brief overview.
Time of the start of therapy
Until recently, people tended to wait too long before using deep brain stimulation. Patients often underwent surgery only after non-motor symptoms had already massively impaired quality of life. A recently published French-German study has shown that deep brain stimulation is superior to drug treatment even in the earlier course of the disease [9]. In this study, the mean age of the patients was 52 years and the mean disease course was seven and a half years. By analogy, the (unpublished) analysis of our own data showed that those patients with the shortest disease course had the most significant response not only in terms of quality of life but also in terms of reduction of motor symptoms.
Literature:
- Bergman H, Wichmann T, DeLong MR: Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science 1990; 249: 1436-1438.
- Benabid AL, et al: Acute and long-term effects of subthalamic nucleus stimulation in Parkinson’s disease. Stereotact Funct Neurosurg 1994; 62: 76-84.
- Limousin P, et al: Effect of parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet 1995; 345: 91-95.
- Deuschl G, et al: A randomized trial of deep-brain stimulation for Parkinson’s disease. N Engl J Med 2006; 355: 896-908.
- Weaver FM, et al: Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: a randomized controlled trial. JAMA 2009; 301: 63-73.
- Sürücü O, et al: Subthalamic deep brain stimulation versus best medical therapy for l-dopa responsive pain in Parkinson’s disease. Pain 2013; 154: 1477-1479.
- Weaver FM, et al: Randomized trial of deep brain stimulation for Parkinson disease: thirty-six-month outcomes. Neurology 2012; 79: 55-65.
- Deep-Brain Stimulation for Parkinson’s Disease Study Group: Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med 2001; 345: 956-963.
- Schuepbach WM, et al: Neurostimulation for Parkinson’s disease with early motor complications. N Engl J Med 2013; 368: 610-622.
- German Neurological Society Guidelines, www.dgn.org.
- Lhommée E, et al: Subthalamic stimulation in Parkinson’s disease: restoring the balance of motivated behaviors. Brain 2012; 135: 1463-1477.









