
The classification of wrinkles according to Glogau, Kreyden and de Maio has consequences for therapy. Therefore, it is important to recognize the different patient groups, make a correct diagnosis and target treatment. The principle is: “technique follows function! The main domain of BTX treatment is the upper third of the face. This is due to the fact that in the upper third of the face, the majority of wrinkles are mimic in nature, lipatrophy plays a role only in the suborbital region, and we have a relatively clear number and arrangement of muscular structures. Frown lines (glabella), worry lines (forehead), and smile lines (lateral eye area) are the most common indications for BTX in the upper third of the face.
“Bei Mir Bistu Shein” (With me you are beautiful), title of a swing piece, Andrews Sisters from the Yiddish musical “Men ken lebn nor men lost nisht” (One could live, but they won’t let us), New York, 1938.
Wrinkles can be classified according to various criteria. The classification makes sense and has therapeutic consequence, as we will see. On the one hand, according to Glogau [1], we distinguish four types of wrinkles with increasing age depending on their severity (Fig. 1):
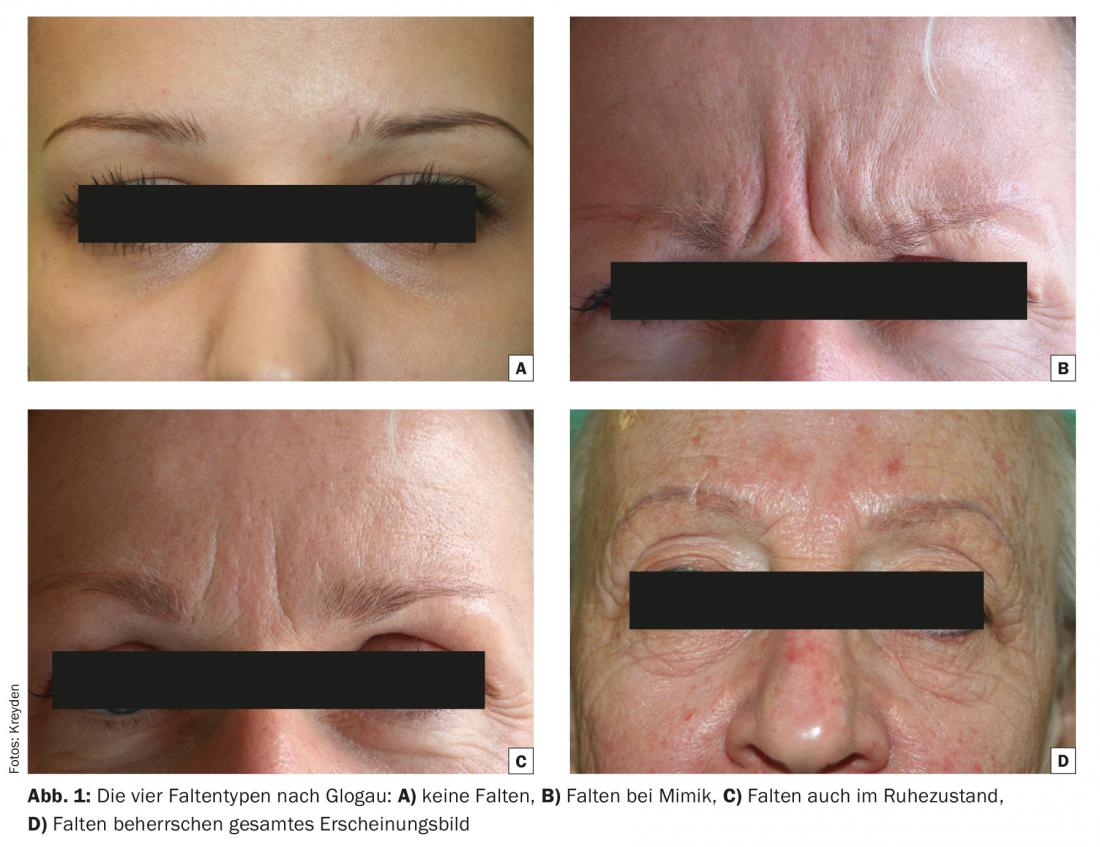
- Type I: No wrinkles
- Type II: Wrinkles with mimic movement
- Type III: Wrinkles even without facial expression
- Type IV: Wrinkles dominate entire appearance.
Another, sometimes more clinically significant, wrinkle classification concerns the etiology of wrinkle development [2] (Fig. 2):
Wrinkles due to mimic hyperfunctionality
Wrinkles due to decreased subcutaneous volume (adipose tissue, musculature, osseous atrophy)
Wrinkles due to cutaneous changes (in the narrow sense actinic elastosis, but also actinic alterations of the skin such as lentigines, actinic keratoses and many others).

Finally, De Maio divides (instead of wrinkles) patients with mimic hyperfunctional facial wrinkles into three groups, which he also wants treated differently [3] (Fig. 3):
- kinetic patients (conscious facial expressions, “I move when I want”)
- hyperkinetic patients (unconscious facial expressions, “victims of involuntary facial expressions”)
- hypertensive patients (persistent facial expressions, “I can’t relax”).

The oldest classification according to Glogau recommends that type I requires no therapy or at most topical therapy. Types II and III are suitable for botulinum toxin treatment, while type IV should rather undergo surgical treatment or deep peeling. This clear classification, which was still valid ten years ago, has been put into perspective somewhat by many years of experience with the drug botulinum toxin (BTX). On the one hand, it has been found that multiple treatments with BTX (and especially with filler treatments) can improve skin appearance and appearance. In addition, it has been shown that improved long-term results are achieved when therapy is started as early as possible. This led to the realization that aesthetic treatments in general and BTX applications in particular should advantageously be performed prophylactically rather than therapeutically first. The kinetic mimic group (equivalent to Glogau I) benefits the most from BTX treatment, as this is where the duration of efficacy is longest. As a prophylaxis, one treatment a year is usually sufficient, regardless of the loss of efficacy after about six months. In the hyperkinetic group, the duration of efficacy is shorter (three to four months) and post-injections to improve clinical outcome are not uncommon. Patients with hyperkinetic facial expressions are the most frequently treated group. The hypertensive patient with a permanent mimic contracture is the most difficult to treat because, on the one hand, the efficacy of BTX is very limited (sometimes only one to two months) and, on the other hand, the frown line usually does not disappear completely. The goal is to move these patients into the hyperkinetic and, at best, the kinetic category. This is often achieved by repetitive treatments up to four times a year. Over time, patients “forget” to contract the muscles and become kinetic patients. This group of patients also suffers disproportionately often from migraine resp. Tension headaches, which are also well addressed with BTX treatment.
BTX is not suitable for every type of wrinkle. This seemingly trivial statement is of considerable importance in everyday clinical practice. It is not uncommon for therapists to attempt to treat non-mimic wrinkles, wrinkles due to a facial volume deficit or due to actinic elastosis, with BTX. This usually stems from the fact that the treating physician is unilaterally educated (“I can only inject BTX according to a given regimen”) or has not made a diagnosis, i.e. has not asked himself what is the cause of the clinical wrinkling. This led to the etiological classification (“technique follows function!”) [2]. BTX can be used exclusively to treat mimic wrinkles, i.e. wrinkles caused by muscular overactivity. If the wrinkles exist due to subcutaneous volume loss caused by lipatrophy, in advanced cases even osseous atrophy, BTX treatment will not improve, in most cases even worsen the clinical picture. Examples include suborbital wrinkles due to lipatrophy in the cheekbone area. If BTX is used, the result is unsightly bags under the eyes, as the orbicularis occuli muscle is still the only retaining structure. Patients with actinic elastosis (Glogau IV) also do not benefit from BTX treatment because the underlying wrinkling is due to structural skin changes. For this reason, this group of patients requires refreshment of the skin itself (peeling, laser treatment), and possibly surgical intervention.
In summary, it can be stated that a clinical consequence is derived from the different wrinkle classifications and that it is of great importance to recognize the different patient groups in advance so that the correct treatment can be carried out after a correspondingly correct diagnosis has been made (“technique follows function!”).
Application of botulinum toxin in the upper third of the face
To anticipate: The domain of BTX treatment is the upper third of the face. This is due to the fact that in the upper third of the face, the majority of wrinkles are mimic in nature, lipatrophy plays a role only in the suborbital region, and we have a relatively clear number and arrangement of muscular structures. The most common indications for BTX in the upper third of the face are:
- Frown lines (glabella)
- Worry lines (forehead)
- Laugh lines (lateral eye area)
Rarer indications, reserved for the more experienced therapists, are eyebrow lifting, the so-called “bunny lines” (wrinkles in the nose), nose tip lifting and facial asymmetries. We will only discuss the main indications below.
Frown lines (glabella): The frown lines are caused by three muscles:
- M. corrugator supercilii: pulls down medial eyebrows
- M. depressor supercilii: pulls medial eyebrows medially
- M. procerus: pulls interocular region downward.
All muscles are so-called depressors, i.e. they pull the facial skin caudally. With a corresponding weakening of the musculature, a lifting effect of the treated area thus occurs. The aim of the treatment is to smooth out the vertical folds in the interocular area (corrugator or depressor supercilii muscle) and the horizontal fold at the root of the nose (procerus muscle). The total BTX amount of approx. 20 units Ona- resp. Incobotulinum resp. 60 units of abobotulinum(see part 1 in issue 1/2015) is distributed over four injections, in the case of co-treatment of the procerus muscle over five injection points (Fig. 4). If the injection points are placed too high, the medial part of the frontalis muscle is treated as well. In this case, there is a medial eyebrow ptosis (with a corresponding tired look) and compensatory lateral eyebrow elevation (“Spock eye” or “Mephisto eyebrows”). A feared complication is eyelid ptosis after treatment of the glabella. This complication does not occur if the needle tip is always placed in the opposite direction to the eye.

Worry lines (forehead): The horizontal forehead wrinkles (worry lines) are the result of increased activity of the frontalis muscle (eye and forehead elevator). Usually this is overused as the patient involuntarily compensates for increasing blepharochalasis. The frontalis muscle is the only muscle that pulls upward in the upper third of the face. This is important in that we must always expect brow ptosis when treating worry lines (forehead treatment, frontalis muscle), especially if the injection points are placed too deep on the forehead. In this case, the result will not be the desired refreshment, but on the contrary, it will result in a tired, depressed-looking facial expression. The patient notices this during daily make-up of the eyelids. Since the eyebrow and thus also the apical part of the upper eyelid are lowered, the application of eye shadow is only possible with the help of a tightening by the non-dominant hand. Clinically, this is easy to test: The patient is instructed to adopt a relaxed facial expression with a forward gaze. With the examining hand, the extent of the forehead sag can be simulated very well and thus the height of the injection points can be determined exactly. In individual cases, however, blepharoplasty must be recommended prior to BTX treatment of the forehead in order to achieve a universally satisfactory result. Depending on the extent of the treatment, six to ten injection points of 2 units of Ona- or Incobotulinum resp. 6 Units Abobotulinum set.
Laugh lines (lateral eyes, “crow’s feet”): There are wrinkles that are more associated with a friendly facial expression and those where the opposite is true. In principle, the superficial, radially arranged wrinkles in the area of the lateral eye area (also unattractively called “crow’s feet”) belong to the “sympathetic” wrinkle formations, especially since they usually only become visible when laughing heartily, which is why the expression “laugh lines” is more appropriate. Especially in light skin types (Fitzpatrick I and II), however, these wrinkles can be aesthetically disturbing. As long as they become visible only mimically, the treatment with BTX is extremely effective. Depending on the extent, three to four injection points of 2 units of Ona- or Incobotulinum, resp. 6 Units Abobotulinum needed to harmonize the lateral eye area. The lateral part of the orbicularis occuli muscle is treated. If the injection points are chosen too deeply, there is a risk of co-impairment of the zygomaticus major and zygomaticus minor muscles. minor. The function of these two muscles is to elevate the upper lip as well as the philtrum. Repeatedly described in the literature as a frequent complication of BTX treatment of the lateral and suborbital region, this complication is de facto negligible. The therapist would indeed have to choose very caudal and very deep his injection points to risk a “frozen smile”.
Treatment of the lower third of the face will be the topic of the next training block. Look forward to it, it will be exciting!
Literature:
- Glogau RG, Matarasso SL: Chemical peels. Trichloroacetic acid and phenol. Dermatol Clin 1995; 13: 263-276.
- Kreyden OP: Botox and men – gender-specific therapy concepts. In: Ruzicka T, et al. (Eds.): advances in practical dermatology and venereology 2008; vol. 21: 452-458.
- De Maio M, Rzany B: Patient Selection. In: De Maio M, Rzany B (eds.): Botulinum Toxin in Aesthetic Medicine. Springer 2007; 11-21.
DERMATOLOGIE PRAXIS 2016; 26(2): 30-33









