A timely correct diagnosis can positively influence the course and treatment options. Auto-antibodies and other serological parameters are diagnostically valuable, but do not have high significance when considered in isolation. To properly classify these and other findings, it is important to always keep the overall context in mind.
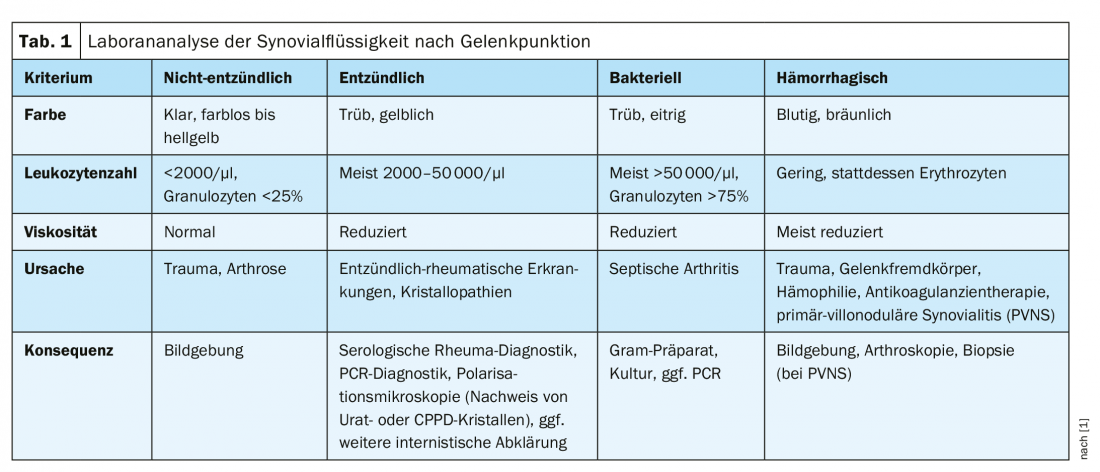
“Joint puncture is a very important tool,” explains Stephan Erni, MD, RehaClinic AG, Bad Zurzach, at this year’s FOMF Basel [1]. The evaluation of the leukocyte count provides information on whether the cause of the disease is non-inflammatory, inflammatory, bacterial or hemorrhagic (Tab. 1). Diagnosis-relevant parameters of serological tests include rheumatoid factors and certain antibodies which are detectable in some forms of rheumatism (e.g. ANCA, ANA, ACPA).
Viewing findings in the overall context
Other informative laboratory tests include determination of the blood sedimentation reaction and acute phase proteins. In addition to synovial fluid analysis and blood tests, imaging techniques may be used and, if necessary, arthroscopy. It is also very important to conduct a careful anamnestic interview, including a survey of the symptom course, relevant previous illnesses and family history.
Relatively frequently, there are referrals with laboratory findings regarding autoantibodies (auto-Ak) with the question of diagnostic relevance, the speaker said. In contrast to causal autoantibodies, associated autoantibodies are a consequence of the pathologic process. ANA, ANF, ENA, RF, and ACPA are among these intracellular antigen-responsive antibodies whose detection makes rheumatologic disease more likely but does not prove it. Conversely, a positive Auto-Ak finding reduces the likelihood of rheumatic disease, but does not exclude it. Autoreactivity per se is not pathological, the decisive factor is the antibody titer. In addition to the classification of the measured values in relation to the respective reference standard values, the pre-test probability plays an important role in the interpretation of the laboratory findings. Therefore, although most auto-Ak are found in diagnostic or classification criteria, they are not mandatory for diagnosis. For a strong significance of Auto-Ak, a high pre-test probability based on clinical pre-clearance is needed, summarizes the speaker [1]. Therefore, he is of the opinion that a determination of auto-Ak at an early stage within the work-up is rather not that useful and a positive auto-Ak finding cannot be interpreted detached from the overall context.
Arthralgia or arthritis?
Joint pain is a cardinal symptom in both arthralgias and arthritides. Unlike arthralgia, in arthritis these are accompanied by classic signs of inflammation (redness, heating, swelling) and are associated with dysfunction. It is also possible that these two clinical pictures occur in parallel in the same patient. If arthralgia or arthritis is suspected, an initial differentiation in the spectrum of possible diagnoses can be made according to the number of affected joints (mono-, oligo-, poly-arthralgias/arthritides, Tab. 2).

Is it gout?
In most gout attacks, symptoms appear within a short period of time in a severe form. “Most gout patients have the greatest increase in pain within the first twelve hours,” said Dr. Erni [1]. It was a helpful anamnestic reference. This should be distinguished from chondrocalcinosis (CPPD) in particular, where multiple to many joints are affected and non-rheumatologic causes (e.g., erysipelas, phlegmon, thrombophlebitis, neuropathic joint deformity) are present.
Löfgren’s syndrome, septic arthritis, or something else?
Löfgren’s syndrome, a subtype of sarcoidosis, is characterized by the triad of erythema nodosum, bihilary lymphadenopathy, and arthritis. Young people are primarily affected. Non-rheumatic DD to consider include granulomatous disease.
Septic arthritis is a highly acute condition with fever, impaired general condition, and elevated CRP levels. The knee joint is most commonly affected, but septic arthritis can also occur in the hip, the speaker adds. Differential diagnoses include crystal arthritis and gout/CPPD. CAVE: Septic arthritis must be recognized and treated quickly, as delay leads to joint destruction!
Reactive arthritis should be considered when symptoms occur in sexually active young adults and acute uro-/entherapathy is present. Enthesitis can be very well differentiated, especially by ultrasound. Dactylitis may be present. Reactive arthritis is also frequently associated with extraskeletal manifestations such as conjunctivitis/uveitis, stomatitis/aphtosis, or erythema nodosum. In addition, anamnestic evidence, for example of previous symptomatic infections (increases likelihood that it is reactive arthritis), is important. If reactive arthritis is diagnosed, antiobiotic treatment is required.
Peripheral spondyloarthritis is characterized by similar symptoms to reactive arthritis, but it does not affect only lower extremities. Comorbidities are often present. One fifth of spondyloarthritides are associated with psoriatic skin manifestations (psoriatic arthritis). In another fifth of cases, inflammation of the intestines occurs (enteropathic spondyloarthritis). Also common is anterior uveitis, usually unilateral, with acute onset and frequent recurrences.
(Activated) osteoarthritis is characterized at an early stage by pain on start-up, fatigue and strain. In a later stage, pain is permanent, increased during movement and at night. Characteristic of (activated) osteoarthritis are also bony thickening and deformation, immobility atrophy of the musculature and stiffening. Various stress factors can act as triggers.
Rheumatoid arthritis is characterized by symmetrical, metacarpophalangeal and peripheral interphalangeal joint involvement; early stage metatarsophalangeal joints are also affected. Typical clinical signs also include morning stiffness (>30 minutes), Gänslen’s test, tendon crepitation, and interosseous atrophy. Often there is an erosive course. Laboratory diagnostic clues include positive rheumatoid factor and ACPA findings.
Viral or infectious in origin?
Viral arthralgias can have a transient to persistent course and often occur concurrently with exanthema. Differentially, differentiation from limb pain is difficult. Viral arthritides frequently occur in the context of the following viral diseases: HBV, parvo, B19, rubella, chikungunya, dengue, mumps, enteroviruses; less frequently in: adenoviruses, (para)influenza, herpes, HIV, HTLV-1.
Streptococcal rheumatism is also called post-streptococcal arthritis but is better known as rheumatic fever, which typically occurs several weeks or months after infection with bacteria of the genus Streptococcus and is often accompanied by angina tonsillaris. Rubor/Dolor/Calor are most pronounced in the region of the large joints. In 50-60% of cases, arthralgias are not accompanied by overt angina. Chorea minor is a possible late consequence of rheumatic fever and is characterized by hyperkinesia and muscle weakness, among other symptoms.
Lyme arthritis is characterized by broad joint manifestations. In particular, septic and reactive arthritis should be distinguished in the differential diagnosis. The following staging is given in the literature: Stage I: Erythema chronicum Migrans, flu-like general condition, hepato-/splenomegaly, IgM after 1-2 weeks; Stage II: Lymphocytoma, facial paresis, Bannwarth syndrome, arthralgias/arthritis, ophthalmologic symptoms, cardiac symptoms; Stage III: Arthritides (Lyme arthritis, jumps from joint to joint), muscle inflammations, bone pain, fibromyalgias, acrodermatitis chronica atrophicans Herxheimer. The speaker mentioned that this staging does not apply to all cases and sometimes there are symptom-free intervals. The most important diagnostic information is contained in the tick bite history.
Literature:
- Erni S: DD of Rheumatology, Stephan Erni, MD, RehaClinic AG, Bad Zurzach, slide presentation, FOMF Basel, Jan 30, 2020.
- Manger B, Schulze-Koops H (eds): Checklist Rheumatology. 4th ed. Stuttgart: Thieme, 2012.
HAUSARZT PRAXIS 2020; 15(5): 40-42 (published 8.5.20, ahead of print).









