Thermal injuries are common and can be momentous. The goals of wound care are low-pain treatment and rapid healing with as few scars as possible. The guideline of the German Society for Burn Medicine published in February 2021 summarizes the most important therapy principles in a separate chapter.
Further topics in the guideline are (pre)clinical initial care, diagnostics, and qualified follow-up of injured skin [1]. The main cause of burns in Central Europe is direct flame exposure, followed by scalds explosion injuries, contact burns and electrical accidents. The remainder are due to other thermal damage such as sun exposure. More than half of burn injury cases occur in the home environment, and about one-fifth are the result of a workplace accident. To achieve an optimal therapeutic goal, any treatment of thermal injuries should be interdisciplinary by practitioners designated in burns. Even burns that are small in area can result in significant scarring. Due to functional and/or aesthetic deficits, scars can cause lifelong stigmatization of affected patients.
Assessment of the degree of combustion
The depth of the burn, along with the localization of the burn and the overall extent, is the most important criterion for selecting the appropriate treatment strategy. The general condition of the patient must always be taken into account. The definitive assessment of the depth of the burn based on the wound bed should be preceded by the removal of any skin blisters that may have formed and the cleaning of the wound of debris.
Clinical assessment of wounds is based on the burn depth criteria (grades 1-4) listed in Table 1. The second-degree burn, in the transition from superficial to deep dermal injury, is difficult to assess clinically, especially in terms of the need for surgery. Therefore, the concept of burning of indeterminate depth was established. Second-degree burns that heal within two weeks have a low risk of developing a hypertrophic scar. If a wound takes more than three weeks to heal, this risk is greatly increased [2].

Local therapy and other measures at a glance
An important treatment goal is to promote the wound healing process and quality of life and to avoid complications. Wound treatment should be as painless as possible. The patient must be informed about the necessary treatment, possible alternatives, risks and complications of the individual therapy procedures.
GRADE 1: Treatment of the first-degree burn should be conservative with nurturing ointments. Antimicrobial treatment is not required topically or systemically. As a rule, a bandage is not necessary. First-degree burns are painful, associated with itching, and characterized by skin redness and edema. Thermal damage affects only the epidermis. Substantial tissue loss does not occur. These injuries usually do not require inpatient therapy [3].
GRADE 2a: Treatment of superficial second-degree burn involves wound cleansing and adequate wound coverage. Wound cleansing with debridement should be performed under aseptic conditions and should be associated with as little pain as possible. Gentle mechanical methods (e.g. brush, sponge) are suitable for debridement of these wounds. The goal of debridement of the superficial second-degree burn is to remove the burn blisters, foreign bodies, contaminants, and wound debris. Contamination and wound debris can interfere with wound healing [4,5]. The use of disinfecting solutions is required for wound cleansing.

Occlusive dressings with inactive, active or biological management systems can be used for subsequent treatment:
- The use of management systems containing silver may be considered.
- Synthetic or biological temporary skin substitutes may also beused.
- Treatment with wound-healing ointments, medicated honey, or antimicrobial ointments, in combination with other wound coverings (e.g., fat gauze) if necessary, may be given, although patients should be advised of the need for repeated, possibly painful, application.
Performing wound checks is recommended until healing occurs. In clinically manifest infection, surgical debridement with removal of infected tissue is advised. Numerous studies have compared the different wound management systems, and no superiority of one system over another has been found with regard to healing time [6].
GRADE 2b: If depth is clearly assigned with a diagnosis of deep second-degree burn, removal of necrotic tissue should be performed, for example, by tangential excision. Enzymatic debridement may be considered for removal of necrotic tissue. The goal of debridement of deep second-degree burn wounds is to remove the necrotic tissue while sparing the vital wound bed. Special instruments developed for burn surgery are available for this purpose [7].
- Enzymatic wound cleansing represents a new interesting technique to gently remove avital burnt tissue [8].
- In the case of infection-free deep second-degree wounds, split-thickness skin grafting should be performed in the same operation if the size and location of the wound and the patient’s condition permit.
- If single-stage split-thickness skin grafting is not possible, the wound should be covered with a sterile temporary skin substitute. In these cases, two-stage autologous split-thickness skin grafting is necessary. If the wound bed is questionable for grafting, it is also recommended to temporarily cover the wound with a sterile management system or skin substitute. Prompt re-evaluation with re-debridement or skin grafting should be considered.
- In the case of deep second-degree wounds, an epifascial necrectomy may be necessary in justified individual cases such as deep wound infection, severely burned patients with limited operability or increased surgical risks due to blood loss, since this method can often be performed more quickly and with less blood loss. Suitable measures to reduce blood loss include tourniquets or topically applied vasoactive substances. If the depth of extension is unclear (2a/2b), it may be considered to perform debridement followed by treatment with temporary skin substitutes or antiseptic dressings and wait until a maximum of three weeks. In the absence of healing, split-thickness skin grafting should then be performed.
GRADE 3: Depending on the size and location of the wound, surgical tangential or epifascial necrectomy should be performed. Tangential necrectomy can also be performed enzymatically in justified cases. Also depending on the size and localization of the wound and the condition of the patient, it is recommended to necrectomize the wounds completely or sequentially in a timely manner. If possible, the defect should be covered by a split-thickness skin graft.
In case of large defects or critical condition of the patient, temporary coverage with skin substitutes can be performed.
- For this purpose, inactive, active or biotechnologically produced management systems as well as biological temporary skin substitutes can be applied. In these cases, two-stage autologous split-thickness skin grafting is necessary. Removal of the banished skin is a prerequisite for undisturbed healing.
Prompt removal of burned skin has shown benefits in terms of morbidity and, in special patient groups, mortality [4]. Early defect coverage by autologous skin grafting also results in reduced morbidity and mortality [9].
- In the case of an extensive burn that cannot be simultaneously necrectomized and split-thickness skin grafting, temporary wound coverage with extraneous skin, low-pressure systems, or other wound management systems is advisable. The aim here is to ensure low-germ wound coverage and minimize fluid loss from the wounds.
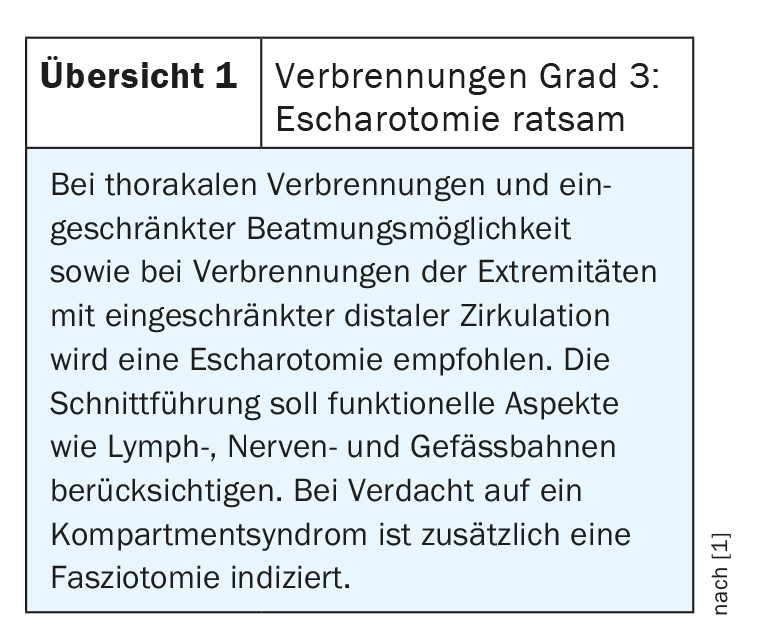
- For scalds or burns to the extremities or neck or trunk that involve at least two-thirds of the circumference or are circular, consider the indication for escharotomy. Here, the current and expected state of swelling and the current perfusion of the affected extremities as well as ventilation parameters must be evaluated (overview 1). The escharotomy circumscribes the incision of the burn scab or the burn wound. It is not necessary to cut through all the subcutaneous fat tissue except for the muscles. If indicated, escharotomy is an emergency procedure.
- The split skin removal site should be discussed with the patient. The split-skin extraction site should be selected from a functional and esthetic point of view. After healing, a new split-skin extraction is possible. Wound coverage of the split-skin donor site should promote healing and consider patient comfort (Box).
- If skin grafting proves necessary, unmeshed or unexpanded grafts should be used on the face, neck, décolleté, and hands. For esthetic and functional reasons, unmeshed grafts should also be considered for other regions. The split skin grafts should be fixed to the wound surface. Various techniques are available for this purpose (box).
Literature:
- DGV: Guideline: treatment of thermal injuries of the adult Class: S2k AWMF-Register-No: 044-001 February 2021.
- Bombaro KM, et al: What is the prevalence of hypertrophic scarring following burns? Burns 2003; 29: 299-302.
- Hartford CE, Kealey GP: Care of outpatient burns. In: Total Burn Care, Third edition, Herndon, DN (Eds) 2007: 67.
- Wilder D and Rennekampff HO: Debridement of burn wounds: rationale and options.Handchir Mikrochir Plast Chir 2007; 39(5): 30.
- Sargent RL: Management of blisters in the partial-thickness burn: an integrative research review. J Burn Care Res 2006; 27: 66-81.
- Wasiak J, et al: Dressings for superficial and partial thickness burns. Cochrane Database Syst Rev 2013; 3:CD002106.
- Rennekampff HO, Tenenhaus M: Debridement of the burn wound. In : Color Atlas of burn reconstructive surgery. Eds Hyakusoku et al, Springer 2010, 10-14.
- Rosenberg L, et al: A novel rapid and selective enzymatic debridement agent for burn wound management: a multi-center RCT. Burns 2014; 40: 466.
- Wolfe RR, Goodenough RD, Wolfe MH: Isotopic approaches to the estimation of protein requirements in burn patients. Adv Shock Res 1983; 9: 81-98.
- Werdin F, et al: Healing Time Correlates With the Quality of Scaring: Results From a Prospective Randomized Control Donor Site Trial. Dermatol Surg 2018; 44(4): 521-527
- Barret J: The role of alternative wound substitutes in major burn wounds and burns scar resurfacing . In: Total Burn Care. Edt Herndon DN. Elsevier4th Edition, 2012.
HAUSARZT PRAXIS 2021; 16(9): 26-29