
Typical of cardiac amyloidosis is the development of heart failure with preserved ejection fraction (HFpEF). New diagnostic procedures and therapeutic options are now shedding a different light on this rare, previously practically incurable disease.
With the advent of new diagnostic procedures and therapeutic options for what has been a virtually incurable rare disease, interest in amyloidosis is growing rapidly. Cardiac involvement (cardiac amyloidosis) usually leads to severe heart failure with all its clinical consequences. The aim of this article is to provide a brief overview of the modern diagnosis and therapy of cardiac amyloidosis.
Origin
In systemic amyloidosis, there are deposits of abnormally folded and aggregated proteins in the tissues. Depending on the organ infestation, corresponding functional disorders and diseases present themselves. If the deposits are in the heart (in the interstitium between the myocardial cells), this leads to heart disease with the clinical picture of heart failure. Two different types of amyloid are usually deposited in the heart, depending on the defective antecedent protein.
AL amyloidosis: This usually develops on the basis of plasma cell dyscrasia. Clonal plasm cells (e.g., in multiple myeloma) produce an excess of free light chains. In the case of amyloidogenic light chains, these are deposited as amyloid fibrils in various organs. Isolated cardiac involvement rarely occurs in AL amyloidosis. Most often, the kidneys, liver and peripheral nervous system are also affected. Lambda light chains are much more frequently detected as amyloid components than kappa chains.
ATTR amyloidosis: Transthyretin (TTR) is a transport protein, 98% of which is produced in the liver and is responsible for thyroxine and rethinol transport. TTR is a tetramer that can dissociate into four monomers. Normally, these monomers are soluble in the blood. However, when dysfunctional, the monomers aggregate to form pathological amyloid fibrils. There are two causes of TTR amyloidosis: The mutant form (hereditary, familial) occurs due to a mutation in the TTR gene. The prevalence of mutations varies by geographic region and ethnic groups. The “wild-type” form (acquired, senile) usually manifests at an older age and predominantly affects the heart.
Clinical manifestation
Cardiac involvement: Typical of cardiac amyloidosis is the development of heart failure with preserved ejection fraction (HFpEF). Amyloid deposition causes the walls of the ventricles and atria to become thicker (no actual hypertrophy, as the myocardial cells per se are not affected). This leads to “stiffening” of the heart and limitation of relaxation (diastolic dysfunction). Thus, there is an increase in end-diastolic filling pressures in the ventricle, dilatation of the atria, and an increase in pulmonary pressure. Clinically, this ultimately leads to left and right heart failure with dyspnea, performance intolerance, and edema. It is also typical that the stiff ventricle can no longer properly adjust the cardiac output. Because of the stroke volume fixed by stiffness, cardiac output is virtually controllable only by heart rate. Syncope and severe orthostatic dysregulation may therefore occur, particularly during exercise, especially in patients taking beta-blockers.
The enlarged left atrium is a “good” substrate for the development of atrial fibrillation. Elevated pressures, together with low mobility of the atrium due to amyloid deposits, may lead to an increased risk of intra-atrial thrombi and explain the markedly increased risk of cerebral infarction in amyloidosis patients.
If the amyloid deposits affect the conduction system, blockages occur, especially AV blockages. Furthermore, the risk of sudden cardiac death is increased due to ventricular arrhythmias (especially ventricular fibrillation and “pulseless electrical activity” – PEA).
Another typical manifestation of cardiac amyloidosis is thoracic pain without finding actual coronary artery disease. On the one hand, small micro-thromboses in the microcirculation can trigger angina pectoris (spasms); on the other hand, impaired endothelial function reveals microvascular dysfunction.
Involvement of other organs: The frequent orthostasis problem in amyloidosis patients is mostly caused by damage to the peripheral nervous system and the associated reduced vasoconstriction of the peripheral vessels.
Disturbed intestinal innervation can lead to passage disorders, bloating, abdominal pain and stool irregularities. Renal involvement is usually manifested by proteinuria and a decrease in renal function.
Deposits of amyloid in the GI tract occasionally lead to malabsorption, weight loss, and increased liver stiffness. In AL amyloidosis, the pathognomonic signs of periorbital hemorrhage and macroglossia may occasionally (10%) be found. TTR amyloidosis is often preceded by carpal tunnel syndrome.
Diagnostics
A variety of diagnostic procedures are used when cardiac amyloidosis is clinically suspected. Peripheral low voltage (attenuation of electrical conduction to the electrodes due to amyloid deposition) is often seen on the ECG, a distinguishing feature from hypertrophic cardiomyopathy, where enhanced voltage is usually seen. Block images, atrial fibrillation and other arrhythmias can also be seen. However, all these changes are not specific to the disease. In the laboratory, the cardiovascular biomarkers NT-proBNP and troponin in particular should be measured in addition to the usual parameters. A urine examination, especially with the question of albumin and urine must also not be missing. Protein electrophoresis and immunofixation in serum and urine is also indispensable to distinguish the AL and ATTR forms.
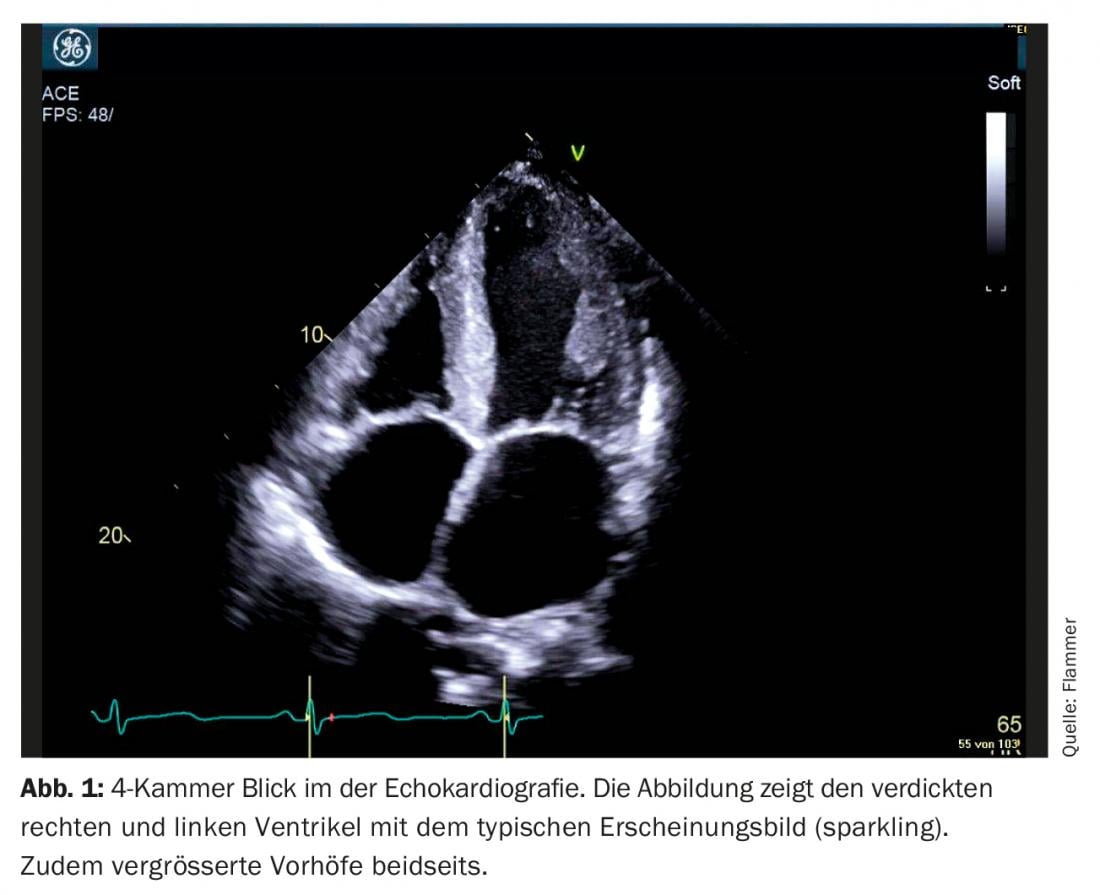
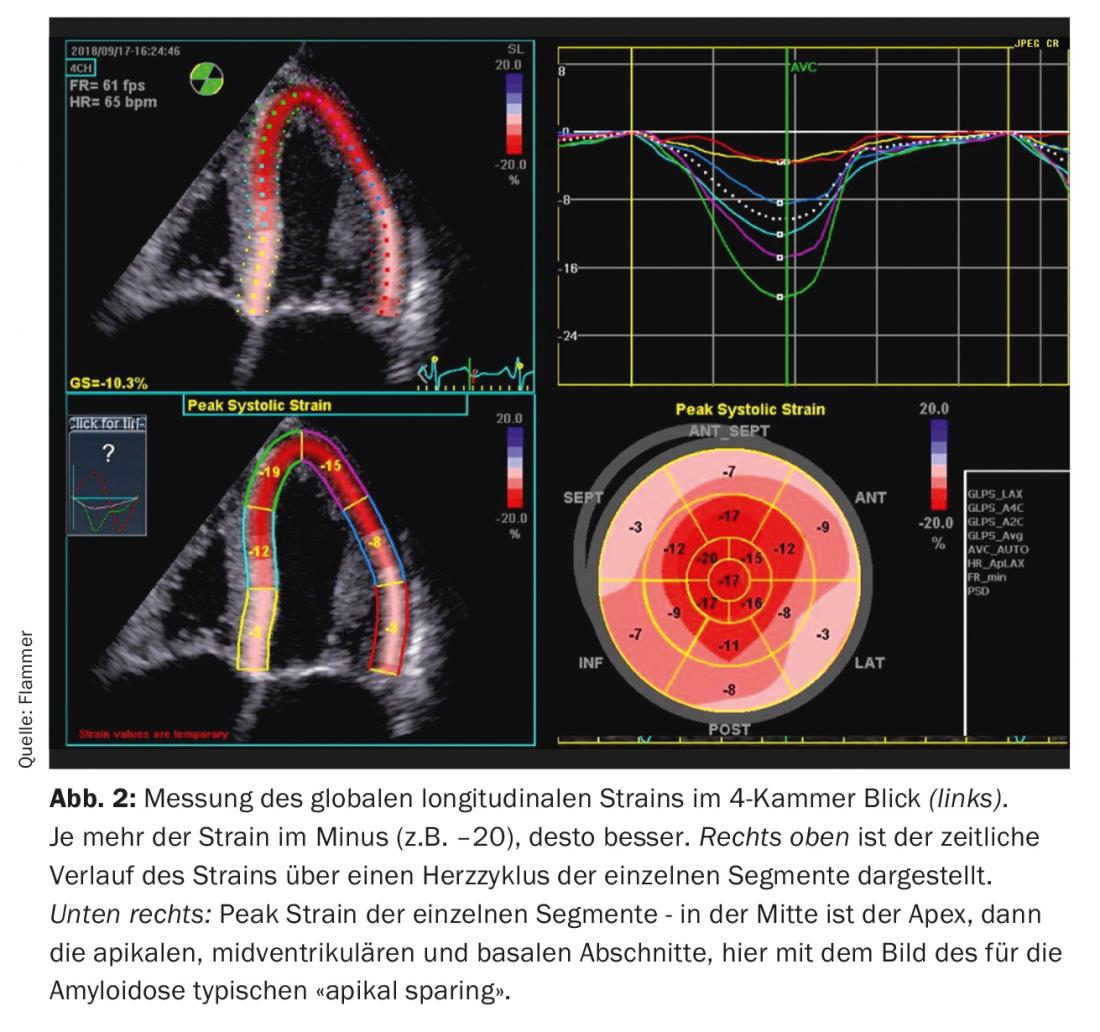
Echocardiography: the diagnosis of cardiac amyloidosis is unthinkable without cardiac imaging. Patients with a history and signs of heart failure usually receive echocardiography. If there are appropriate signs of amyloidosis on echo and manifest heart failure, amyloidosis must be considered. What are typical signs in echocardiography? Biventricularly thickened myocardium is seen, and the intraatrial septum and atrial walls are usually thickened as well. The myocardium also presents specifically as “sparkling”, which is characteristic of the disease (however, it should be remembered that “second harmonic imaging” must be turned off on the ultrasound machine). Amyloid is also deposited on the valves. Thus, these appear slightly thickened, but the function of the valves is usually normal. A discrete pericardial effusion is also frequently found (Fig. 1). Functionally, severe diastolic dysfunction is seen, especially in advanced disease, usually with a restrictive filling pattern. Due to the associated elevated diastolic pressures, both atria enlarge during the course of the disease (biatrial dilatation) – characteristic of severe diastolic dysfunction. Although the ejection fraction is usually normal, systolic dysfunction is also evident, which is manifested by decreased “strain” (strain describes the measured deformation of the myocardium). In particular, the global longitudinal “strain” is limited. Typical and specific for amyloidosis is the so-called “apical sparing”, i.e. the strain is normal (spared) in the apex but deteriorates the further one goes towards the base of the heart (Fig. 2).
Magnetic resonance imaging (MRI): Nowadays, amyloidosis is frequently diagnosed by this examination (sometimes as incidental findings in other investigations). The changes seen on MRI are similar in principle to those seen on echo, but additional typical changes may be seen, especially if the contrast agent gadolinium is also used. Due to a slow “wash-out” of gadolinium, it remains longer in interstitium if amyloid is present there. MRI then shows diffuse and patchy “late gadolinium enhancement” typical of amyloidosis.
Diagnostic algorithm for suspected cardiac amyloidosis.
In patients with appropriate clinical presentation and imaging suspicion of cardiac amyloidosis, plasma cell dyscrasia must be excluded in the first instance. For this, protein electrophoresis and immunofixation must be sought in urine and serum as described above. If one is present, the primary search is for AL amyloidosis, and in the absence of signs, ATTR amyloidosis (Fig. 3).
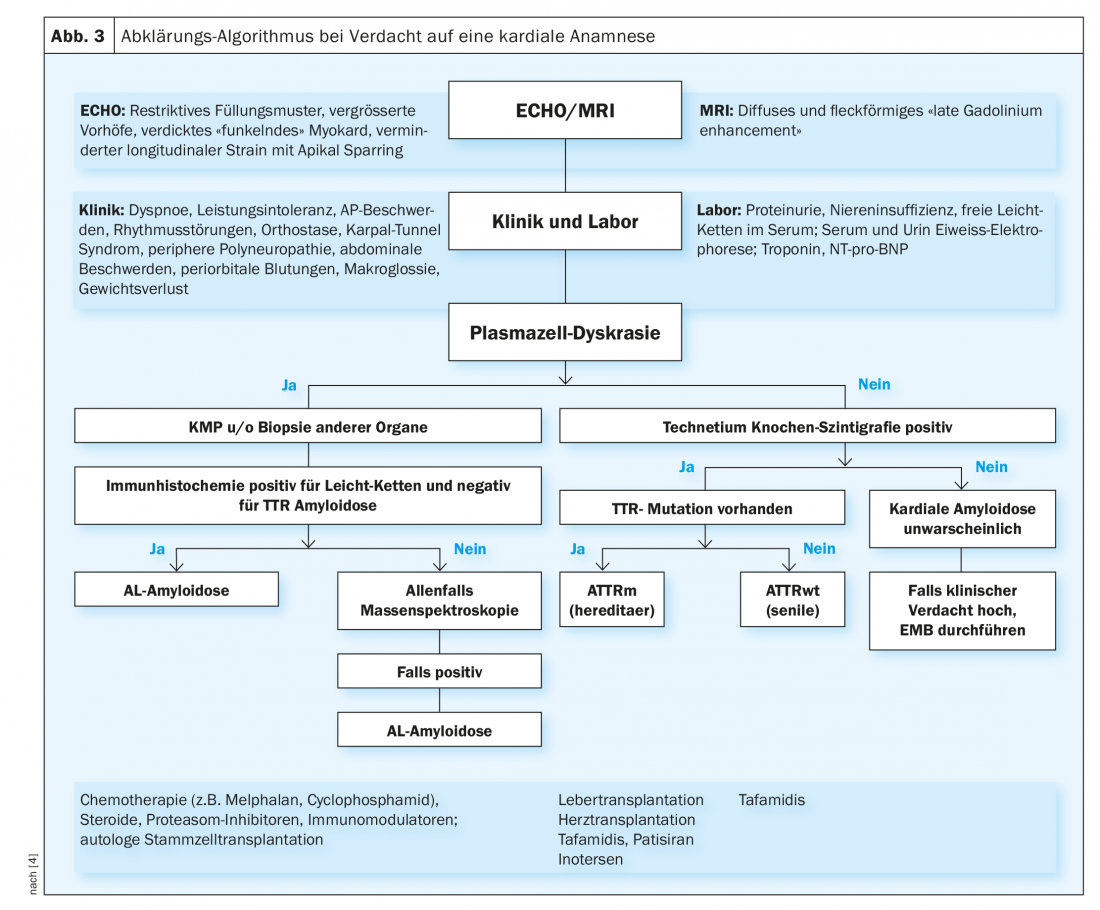
If AL amyloidosis is suspected (plasma cell dyscrasia present), an attempt must be made to detect AL amyloid directly biotopically. Bone marrow aspiration is usually performed to diagnose the underlying hematologic disease (usually multiple myeloma). Since amyloidosis is a systemic disease, the diagnosis is confirmed as soon as AL amyloid is detected in a biopsy (of any tissue). Aspiration of abdominal adipose tissue is the least invasive and traumatic. Also, amyloid can sometimes be looked for in previously performed tissue sampling during colonoscopy or gastroscopy. Further, salivary gland, lip, or rectal biopsies can be performed. Occasionally, renal or endomyocardial biopsy is also necessary to make a definitive diagnosis. In cardiac amyloidosis, endomyocardial biopsy is very sensitive. On the one hand, the biopsies are examined for amyloid, and on the other hand, immunohistochemistry is used to try to classify the type of amyloidosis. In difficult cases, mass spectroscopy (gold standard) is necessary. However, only a few pathologies perform such an examination at all.
If TTR amyloidosis is suspected (lacking evidence of plasma cell dyscrasia), technetium (bone) scintigraphy is nowadays performed. Under these conditions, the sensitivity and specificity of this methodology in cardiac ATTR amyloidosis is very good. Therefore, if positive, a biopsy can be omitted and the diagnosis made. If the scintigraphy is unclear and cardiac amyloidosis remains suspected, an endomylocardial biopsy should be obtained at this site.
Once ATTR amyloidosis is confirmed, genetic testing is needed to distinguish whether a “wild-type” or hereditary form is present.
Therapy of cardiac amyloidosis
Heart failure is usually at the center of symptomatology in cardiac amyloidosis. Therapeutically, these must be addressed first and foremost. Symptomatically, diuretics help further. Especially since cardiac filling pressures are elevated due to restrictive cardiac physiology, leading to passive venous pulmonary pressure elevation. Patients are significantly less symptomatic under diuretics. In the course of the disease, higher and higher doses are usually needed – accordingly, care must also be taken to ensure that sufficient potassium is substituted. Titration of the dose is often challenging (box).
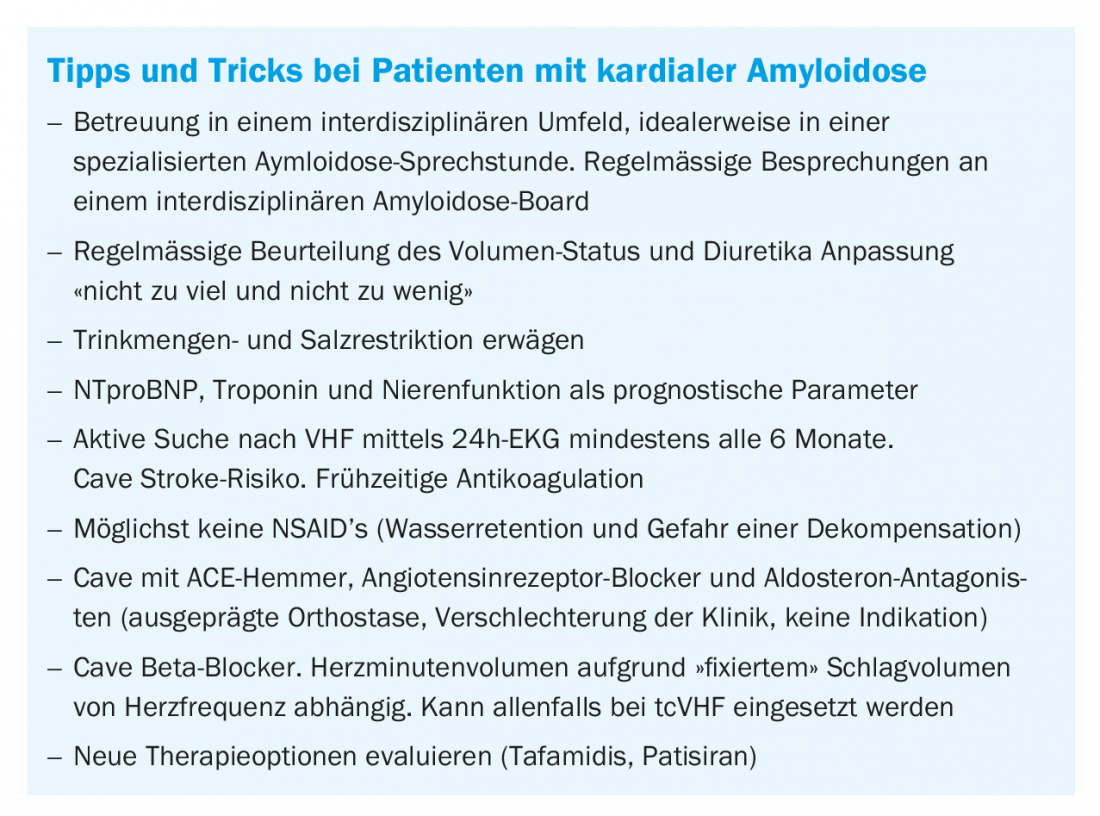
According to HFpEF physiology, there is no indication for ACE inhibitors, beta-blockers, and aldosterone antagonists. On the contrary, ACE inhibitors in particular can exacerbate what is often already marked orthostasis. Beta-blockers result in the inability to increase cardiac output under stress due to the fixed stroke volume. Thus, beta-blockers are withheld for patients in tachycardic atrial fibrillation.
Atrial fibrillation and cerebral infarctions as a result, are common. On the one hand, it is essential not to miss VHF (6-monthly Holter examinations), and on the other hand, oral anticoagulation must be initiated if present, regardless of CHADS-Vasc score. It is not completely clear whether OAK should be started in the absence of VHF – it is probably reasonable if the filling pattern is restrictive. In tachycardic VHF, rate control with beta-blockers should be performed; digoxin should not be given because of increased toxicity. Amiodarone is indicated in certain patients for rhythm control and occasionally for rate control.
Due to the disturbances in the cardiac conduction system, pacemaker implantation becomes necessary, especially in patients with TTR amyloidosis, an indication which can be given generously. The question of whether to implant an implantable cardioverter defibrillator (ICD) is particularly challenging. The most common cardiac cause of death in patients with amyloidosis is sudden cardiac death due to ventricular arrhythmias. Not only ventricular fibrillation is observed, but also a relevant number of PEAs. The latter are not reliably detected by an ICD. There is also a higher rate of incorrectly applied shocks (which is very traumatic for patients) and unsuccessful shock deliveries. So far, there are only retrospective studies on this topic, which show no clear benefit for an ICD. The indication should therefore be made cautiously and discussed in detail in an amyloidosis team.
Causal therapy
In AL amyloidosis, the hematologic disease must be addressed first and foremost. However, this is often challenging, especially in severe cardiac involvement and concomitant severe heart failure. High-dose therapy with autologous stem cell transplantation, which is often targeted, cannot be performed in this case. The other therapeutic regimens with chemotherapeutic agents (e.g., melphalan, cyclophosphamide), steroids, and novel proteasome inhibitors, immunomodulators, or anti-CD38 antibodies can also occasionally be stressful to the heart. However, there are curative approaches in some cases. However, a detailed treatment would go beyond the scope of this article.
For hereditary TTR amyloidosis, liver transplantation (and in advanced stages, heart transplantation) remains the treatment of choice.
However, since summer 2018, two drugs have been available in the US and Europe (FDA and EMA approval) that use RNA interference techonology to ‘silence’ the defective gene so that no amyloidogenic TTR is produced. Neither drug has yet been approved in Switzerland. A large-scale study in patients with hereditary amyloidosis impressively showed how polyneuropathy (which is often prevalent in hereditary amyloidosis) can be stopped. Subgroup analyses on the drug patisiran indicate that cardiac outcomes may be similar, but further studies remain to be seen. Until recently, there was no causal therapy for wild-type TTR amyloidosis. Fortunately, a study also published in the summer of 2018 showed that tafamidis, a transthyretin stabilizer that is also approved in Europe and the United States for the treatment of hereditary amyloid neurpathy, had good results in cardiac amyloidosis with improvement in quality of life, reduction in mortality, and reduction in cardiac-related hospitalizations. The drug is currently not yet available in Switzerland, but approval is expected soon due to the good results.
Take-Home Messages
- AL amyloidosis is a rare disease, which is usually triggered by an underlying hematologic “light chain-producing” disease and often affects other organs besides the heart. At the heart of therapy is the treatment of hematologic disease.
- TTR amyloidosis can be caused by a mutation in the TTR gene or can be “acquired” during life (“wild-type”). The rarer familial form predominantly manifests with polyneuropathy or cardiopathy (or combination), depending on gene involvement; the “wild-type” form is usually confined to the heart. In addition to symptomatic therapy, there are promising new therapeutic approaches using TTR stabilizers and RNA interference molecules.
- The diagnosis of cardiac amyloidosis requires an appropriate clinic (heart failure), echo or MRI findings typical of amyloidosis, and either evidence of amyloid in a biopsy or a positive Tc scintigraphy.
- The typical clinic of cardiac amyloidosis includes, in particular, symptoms of heart failure, orthostasis, syncope, arrhythmias (especially VHF and ventricular tachycardia/ventricular fibrillation), AV block, and microvascular angina.
Literature:
- Brouwers S, et al: Cardiac amyloidosis Cardiovasc Med. 2018; 21(11): 282-289.
- Rauch PJ, et al: Systemic amyloidoses Switzerland Med Forum 2014 14; 943-948.
- Laptseva N, et al: Cardiac amyloidosis: still challenging Eur Heart J 2017, 38(22): 122.
- Falk RH, et al: AL (Light-Chain) Cardiac Amyloidosis: A Review of Diagnosis and Therapy.
- Gillmore JD, et al: Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis Circulation 2016: j133(24): 2404-2412.
- Maurer MS, et al: Tafamidis Tratment for Patients with Transthyretin Amyloid Cardiomyopathy N Engl J Med 2018; 379(11): 1007-1016.
- Adams D, et al: Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis N Engl J Med 2018; 379(1): 11-21.
CARDIOVASC 2019; 18(2): 6-10









