Patients with chest pain require emergency evaluation for acute coronary syndrome (ACS). Diagnostic cornerstones of ACS are clinical presentation, 12-lead ECG, and cardiac troponins. The 0/1 h algorithms recommended as class IA are based on highly sensitive troponin assays and allow safe “rule-out” and accurate “rule-in” of acute myocardial infarction in >70% of affected patients.
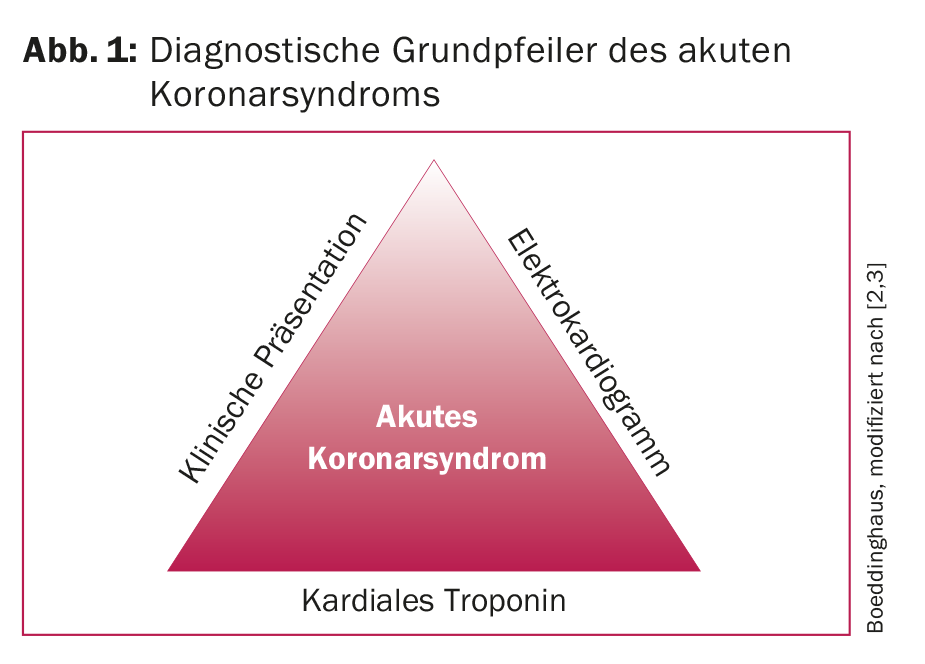
Diseases of the cardiovascular system, such as acute coronary syndrome (ACS), remain the leading cause of death worldwide. Approximately ten percent of all emergency department consultations are by patients with chest pain [1]. Rapid and adequate identification of those patients suffering from acute myocardial infarction (AMI) is essential for the immediate initiation of adequate and evidence-based therapy. Rapid and reliable exclusion of an AMI (the so-called “rule-out”) and rapid and accurate inclusion (the so-called “rule-in”) remain critical challenges for clinicians. Clinical presentation, electrocardiogram (ECG), and cardiac troponins form the three basic diagnostic pillars (Fig. 1) [2,3]. While ECG is the diagnostic tool of choice for detecting ST elevation myocardial infarction (STEMI), cardiac troponin plays the critical role in diagnosing non-ST elevation myocardial infarction (NSTEMI). In this article, we would like to give you an overview of the optimal workup for cardiac-related chest pain. The focus is on early detection of AMI, which carries the highest morbidity and mortality among the differential diagnoses associated with chest pain and requires immediate therapy.
The clinical presentation
The symptomatology of patients with chest pain can be divided into typical and atypical angina pectoris (AP) symptoms. In general, it is important to emphasize that the concept of typical, atypical, and noncardiac thoracic pain is not evidence-based, and that one-third of all patients with an AMI do not have typical thoracic symptoms, and as many as half in elderly patients [4]. For typical AP symptoms, the following three criteria must be met:
- Retrosternal feeling of pressure or tightness
- Triggered by physical or mental stress
- Decrease in discomfort due to physical rest
Concomitant vegetative symptoms such as dyspnea, nausea, and vomiting are very common in typical AP complaints. In atypical AP complaints, only two of the above criteria are met. When only one or none of the criteria are met, the condition is referred to as noncardiac thoracic pain.
Stable AP is present when the pain episodes are always the same and the pain subsides at rest or improves after taking preload and afterload lowering medications.
An unstable AP is when the symptoms are new, there is an increase in the intensity or duration of the symptoms, the symptoms recur even at rest or within two weeks of an AMI. Troponin levels are usually within the normal range (or slightly elevated) in unstable AP, compared with NSTEMI, and show no significant dynamics. If an unstable AP is suspected, a workup in a hospital must be performed without delay in order to rule in or rule out an AMI as quickly as possible.
The electrocardiogram
The electrocardiogram (ECG) plays a critical role in the diagnosis of AMI and differentiates between STEMI and NSTEMI. Furthermore, it allows conclusions to be drawn about the localization of the infarct area and the affected coronary vessel. Classic ECG changes suggestive of STEMI are ST elevations in two adjacent leads (I+AVL, II+III+aVF, V1-V6) measured at the J point, with amplitude >0.1 mV. For leads V2 and V3, the amplitude must be >0.15 mV for women, >0.25 mV for men under 40, and >0.20 mV for men over 40. Additional posterior leads, such as V7, V8, V9, or right-sided leads (V3R, V4R) may be helpful in establishing the diagnosis in certain cases (ST depressions above the anterior wall). ECG changes in NSTEMI or unstable AP are varied, although the ECG may be completely unremarkable. Typically, ST depressions or T-wave negativities occur. Rather, Q-spikes are indicative of an older, expired infarct.
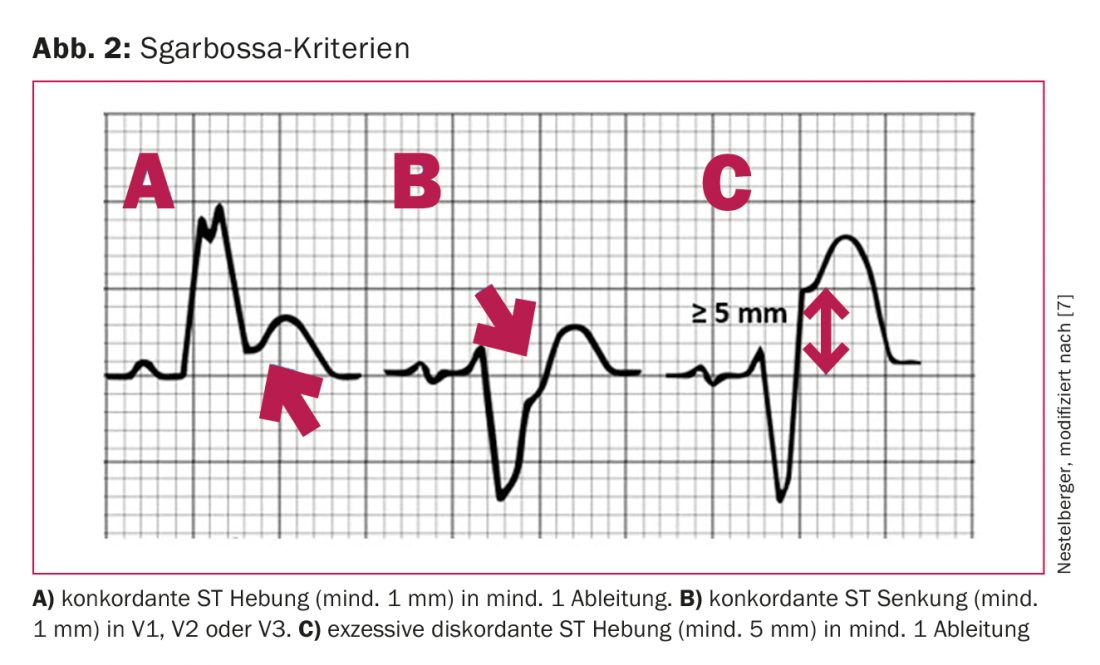
Patients with chest pain and left bundle branch block (LSB) present a special challenge [5]: Current American College of Cardiology guidelines recommend that patients with new or probable new LSB should be treated analogously to STEMI (STEMI equivalent). However, recent studies have shown that the majority of patients with chest pain and LSB do not have AMI. Furthermore, no difference was found between preexisting LSB and new or probable new LSB with regard to AMI prevalence, although evaluation of preexisting ECGs is very often not possible, especially in emergency situations. Thus, an LSB is rather an expression of chronicity in different cardiac diseases (ischemic, valvular, or hypertensive cardiopathies). Recently, specific ECG criteria (called Sgarbossa or modified Sgarbossa or Smith criteria) have been shown to have very high specificity (94-100%) for AMI in LSB (Fig. 2) [6]. Therefore, these specific ECG criteria should be included in the evaluation of LSB ECG’s and only if one of these criteria is present should treatment and further evaluation by immediate coronary angiography be performed.
The cardiac troponin
Cardiac troponin is a protein complex consisting of three subunits: troponin C (calcium-binding), troponin T (tropomyosin-binding), and troponin I (inhibitory subunit). Cardiac troponin T and cardiac troponin I are heart-specific and have served for decades as cardiac biomarkers of myocardial necrosis, which occurs particularly in the setting of AMI.
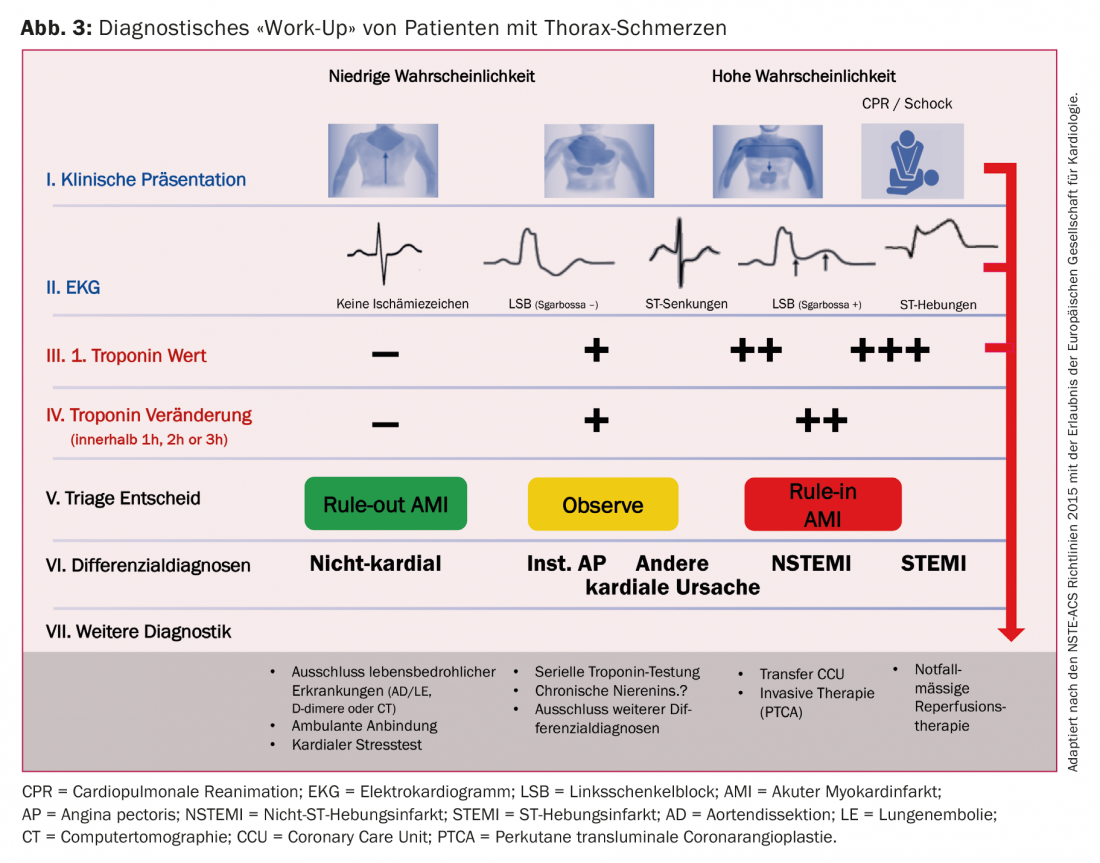
Recent years have seen the development of high-sensitivity troponin (hs-cTn) assays [8,9]. Due to the higher sensitivity, troponin levels, even in the very low normal range, can now be detected in more than 50% of a healthy population. The “troponin-blind” interval of the assays is thus reduced and the diagnostic accuracy of the hs-cTn assays is significantly higher than that of older generation assays. The development and clinical use of hs-cTn assays has significantly changed the clinical interpretation of troponin. The terms “troponin positive” or “troponin negative” no longer reflect the current state of medical knowledge. It is well known and adequately documented that troponin should be used as a quantitative marker. That is, the higher the measurable troponin, the greater the myocardial damage and the corresponding release of cardiac troponins into the peripheral circulation and the higher the risk of future cardiovascular events and mortality during follow-up. The diagnostic “work-up” of patients with chest pain is shown in Figure 3.
Algorithms for inclusion or exclusion of acute myocardial infarction.
Through the use of hs-cTn assays, a variety of algorithms for “rule-out” or “rule-in” of AMI have been developed in recent years [10–14]. Some of these strategies are based solely on troponin values, while others integrate ECG information and/or clinical risk scores. Two of these new algorithms, the 0/1 h algorithm and the 0/3 h algorithm, were included as class IA recommendations in the European Society of Cardiology guidelines. Two 0/1 h algorithms have been developed for the two established and clinically available hs-cTn assays (hs-cTnT Elecsys and hs-cTnI Architect) and have so far been validated exclusively for emergency department use (Figs. 4A and 4B). Their use in the outpatient setting, e.g., in family practice, is not possible at this time because no hs-cTn assays are available in the outpatient setting, only the much less sensitive point-of-care assays.
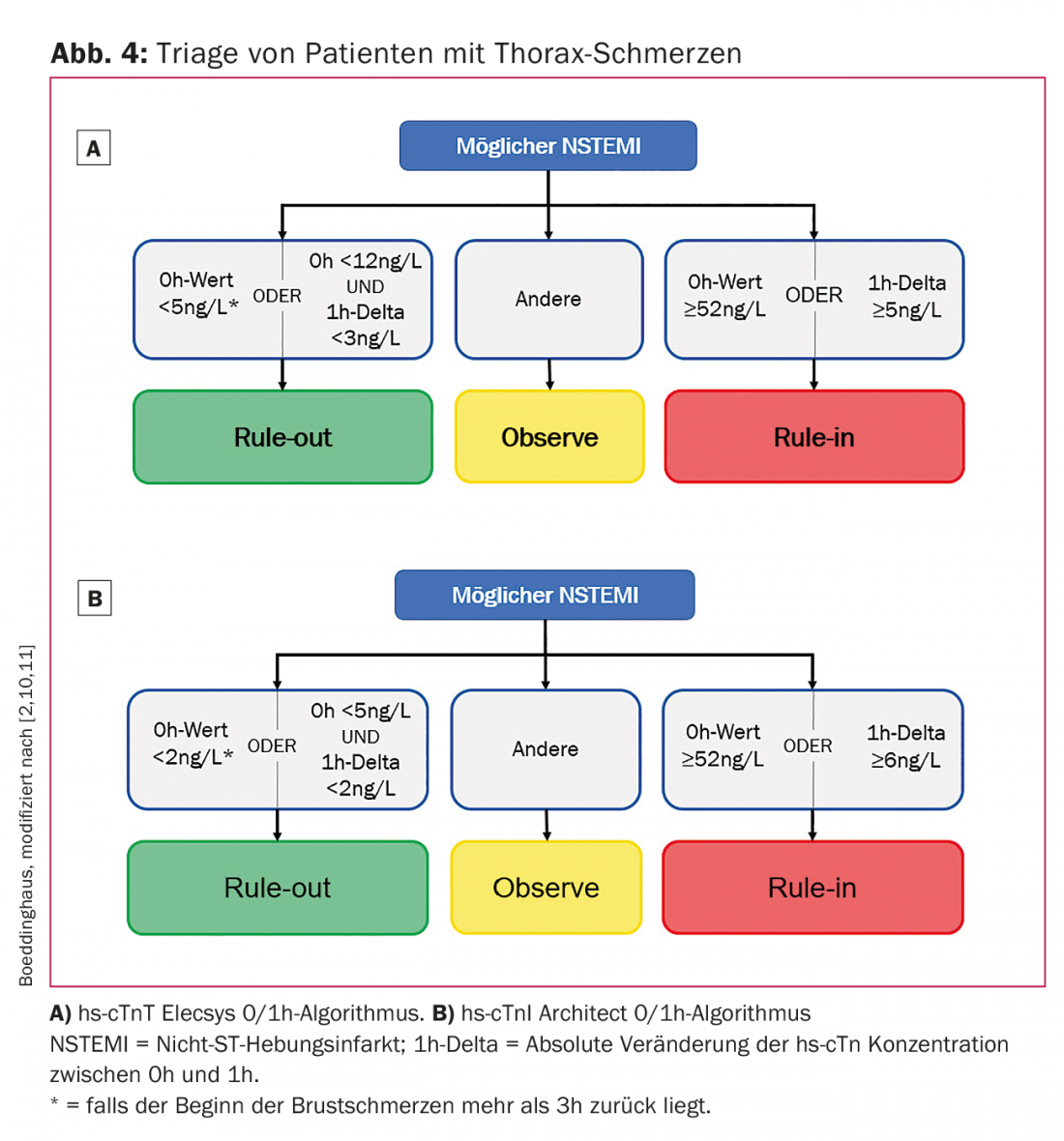
The algorithms use absolute hs-cTn concentrations at presentation and after 1 h and 3 h after presentation, respectively. Also used are the absolute changes (called delta) between first and second troponin measurements. The 0/1 h algorithms classify patients as rule-out if they have low hs-cTn concentrations at presentation and if the absolute change is below a certain value within the first hour. A direct “rule-out” based on a very low troponin value is possible if the onset of pain at the time of blood sampling was at least 3 h ago. The 0/1 h algorithms show high certainty for rule-out with a resulting sensitivity and negative predictive value of >99% [10,11]. For “rule-in,” patients need either very high hs-cTn levels at presentation to the emergency department, or a significant change in hs-cTn concentrations. Four aspects need to be considered regarding the clinical application of these troponin-based algorithms. First, all algorithms should always be used in combination with the overall clinical information and individual pretest probability for an AMI. Second, the algorithms addressed should be understood as triage strategies rather than diagnostic strategies, as they do not diagnose AMI but rather divide patients into three groups. Subsequently, further diagnostics, such as coronary angiography, stress tests, or echocardiography, may be necessary until a diagnosis is made (Fig. 3). Third, all algorithms should always be applied only after a STEMI has been ruled out by ECG, because patients with a STEMI require emergency reperfusion therapy. Fourth, the algorithms should be integrated into standard local emergency department procedures to ensure the smoothest possible application.
Summary
Rapid and reliable diagnosis of ACS in patients presenting with chest pain remains a major challenge. Emergency evaluation in a hospital, ideally with an available catheter laboratory, is mandatory. The development of hs-cTn assays and the corresponding 0/1 h algorithms is certainly the greatest achievement in early diagnosis of ACS in recent years. The distinction between an AMI and an unstable AP by the use of hs-cTn assays is of great relevance, because unstable AP is a much more harmless disease compared to AMI, which usually does not require rhythm monitoring and emergency coronary angiography. By using the newly developed algorithms, it is possible to classify approximately 70% of all patients as “rule-out” or “rule-in” within a very short time [10,11]. As a result, patients with ACS can be directed to evidence-based therapy even more quickly. On the other hand, the majority of patients can be discharged home with a very high degree of safety and, if necessary, receive outpatient follow-up care. As a result, the length of stay in the emergency ward is significantly reduced, and the stress for patients, relatives, and also for medical staff is reduced. Likewise, faster diagnosis of ACS prevents overcrowding in emergency departments and ultimately leads to a sustainable reduction in healthcare costs.
Take-Home Messages
- Diseases of the cardiovascular system, such as acute coronary syndrome, remain the leading cause of death worldwide.
- Patients with chest pain require emergency workup for acute coronary syndrome.
- The basic diagnostic pillars of the acute coronary syndrome are
- The clinical presentation, 12-lead electrocardiogram, and cardiac troponins. All information should always be included in the diagnosis.
- The clinical introduction of high-sensitivity troponin assays was a milestone in the early diagnosis of acute myocardial infarction and enabled the development of troponin-based algorithms.
- The 0/1 h algorithms recommended as class IA by current guidelines allow safe “rule-out” and accurate “rule-in” of acute myocardial infarction in more than 70% of affected patients.
Literature:
- Pitts SR, et al:National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Report 2008; (7): 1-38.
- Roffi M, et al: 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016; 37(3): 267-315.3.
- Thygesen K, et al: Third universal definition of myocardial infarction. Eur Heart J 2012; 33(20): 2551-2567.
- Canto JG, et al: Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA 2000; 283(24): 3223-3229.
- Neeland IJ, Kontos MC, De Lemos JA: Evolving considerations in the management of patients with left bundle branch block and suspected myocardial infarction. J Am Coll Cardiol 2012; 60(2): 96-105.
- Nestelberger T, et al: Diagnosis of Acute Myocardial Infarction in Patients Presenting with Left Bundle Branch Block in Three Prospective International Observational Studies, under Review.
- Sgarbossa EB, et al: Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med 1996; 334(8): 481-487.
- Reichlin T, et al: Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med 2009; 361(9): 858-867.
- Keller T, et al: Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med 2009; 361(9): 868-877.
- Reichlin T, et al: One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch Intern Med 2012; 172(16): 1211-1218.
- Rubini Gimenez M, et al: One-hour rule-in and rule-out of Acute Myocardial Infarction Using High-sensitivity Cardiac Troponin I. Am J Med 2015; 128(8): 861-870.e4.
- Reichlin T, et al: Two-hour Algorithm for Triage Toward Rule-out and Rule-in of Acute Myocardial Infarction Using High-sensitivity Cardiac Troponin T. Am J Med 2015; 128(4): 369-379.e4.
- Boeddinghaus J, et al: Two-Hour Algorithm for Triage toward Rule-Out and Rule-In of Acute Myocardial Infarction by Use of High-Sensitivity Cardiac Troponin I. Clin Chem 2016; 62(3): 494-504.
- Boeddinghaus J, et al: Direct Comparison of Four Very Early Rule-Out Strategies for Acute Myocardial Infarction Using High-Sensitivity Cardiac Troponin I. Circulation 2017; 135(17): 1597-1611.
CARDIOVASC 2017; 16(4): 8-12