There is news in the therapy of mild to moderate asthma, which has already found its way into the GINA recommendations. It’s about using not just a so-called reliever anymore, but a drug with a controller potential as an on-demand drug.
It’s about using not just a so-called reliever anymore, but a drug with a controller potential as an on-demand drug. Patients with mild symptoms are by far the largest group in asthma. “It has been a bit of a sour note for us for quite some time that in this mild to moderate form, the treatment with a bronchodilator, i.e. with a SABA, which is carried out in the overwhelming majority of those affected, can have very unpleasant consequences for quite a few patients,” explained Professor Roland Buhl, MD, III Medical Clinic, Focus on Pneumology, Mainz University Hospital. Even in people with very mild disease and very few symptoms, severe exacerbations and even deaths can still occur.
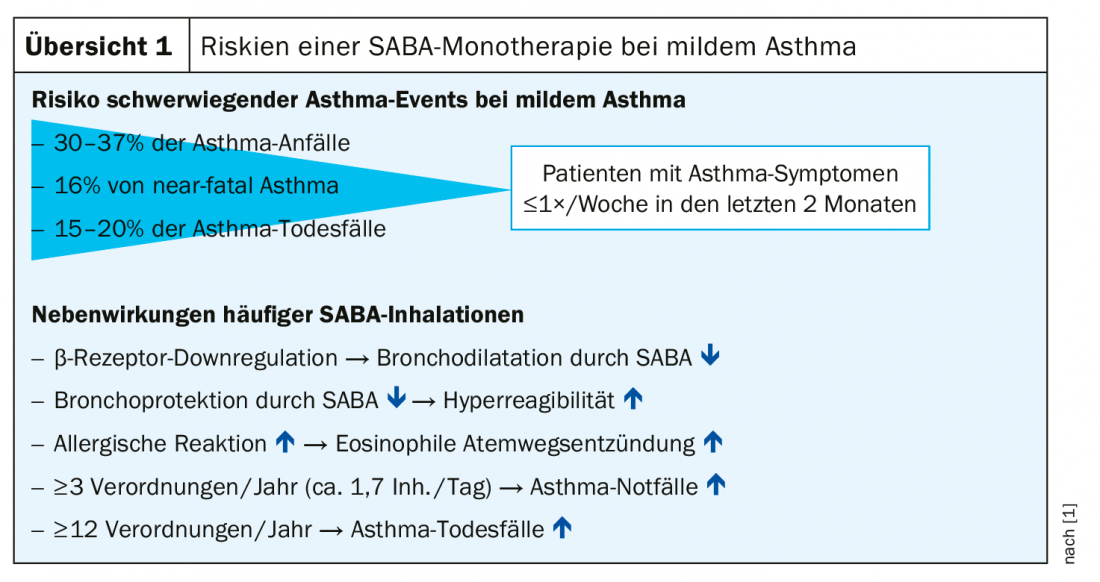
One of the problems from the expert’s point of view: If these patients get complaints and then just reach for the beta-mimetic, they often achieve the exact opposite effect of what was supposed to happen. “We all learned the principle in pharmacology at university: the more frequently a patient uses beta-mimetics, the less effective they become.” The correlation is obvious – the more prescriptions of betamimetics, the higher the risk for patients to suffer severe exacerbations (overview 1).
Formoterol with the same onset of action as salbutamol
For this reason, the idea of adding a very low dose of an inhalable steroid (ICS) to a bronchodilator was developed a few years ago to gently convince the patient to take a low dose of a steroid in addition to an immediate symptom-relieving medication. In the early 1990s, such a drug already existed, recalled Prof. Buhl: salbutamol, a fixed combination of an inhalable cortisone and a betamimetic. “We hardly ever used that – today because of ridiculous fears, which were perfectly understandable at the time, that you could give too much steroid.” The manufacturers have therefore withdrawn the drugs from the market again, except in a few countries, so that there is currently no fixed combination of ICS and short-acting betamimetic. However, some fixed combinations of ICS and long-acting betamimetics did.
Formoterol, for example, has an equally rapid onset of action as salbutamol, and medications containing formoterol can theoretically be prescribed as needed. “That’s the new concept,” said Prof. Buhl: “When a patient has complaints – and only then – he takes his ICS/formoterol medication. If he feels better after a short time, he takes it off again, and if it gets worse again weeks or months later, he takes it again. And in between, he does nothing!”
This concept was tested in the SYGMA studies. Compared were
- only one SABA if needed (until recently guideline recommendation) or
- ICS+SABA as permanent therapy (only very few do this) or
- ICS/formoterol as needed (new).
The result showed that as-needed and continuous use of inhaled cortisone were absolutely equal in their effects when looking only at what is ultimately relavant for patients, namely the effect in severe exacerbations. Clearly outnumbered was only SABA alone.
However, as convincing as the results of controlled clinical trials may be, the question arises as to whether they are transferable to daily clinical practice. The results of the SYGMA studies were therefore verified in an open real-life study.
In a 52-week, randomized, open-label clinical trial in adults with mild asthma, patients were initially randomized to one of three treatment options:
- Salbutamol (100 μg, 2 inhalations from a metered-dose inhaler) only as needed for asthma symptoms (salbutamol study arm),
- Budesonide (200 μg, 1 inhalation by dry powder inhaler 2× daily) plus salbutamol only as needed (budesonide maintenance therapy study arm) or
- Budesonide/formoterol fixed combination (200 μg budesonide/6 μg formoterol, 1 inhalation by dry powder inhaler only when needed; budesonide/formoterol study arm).
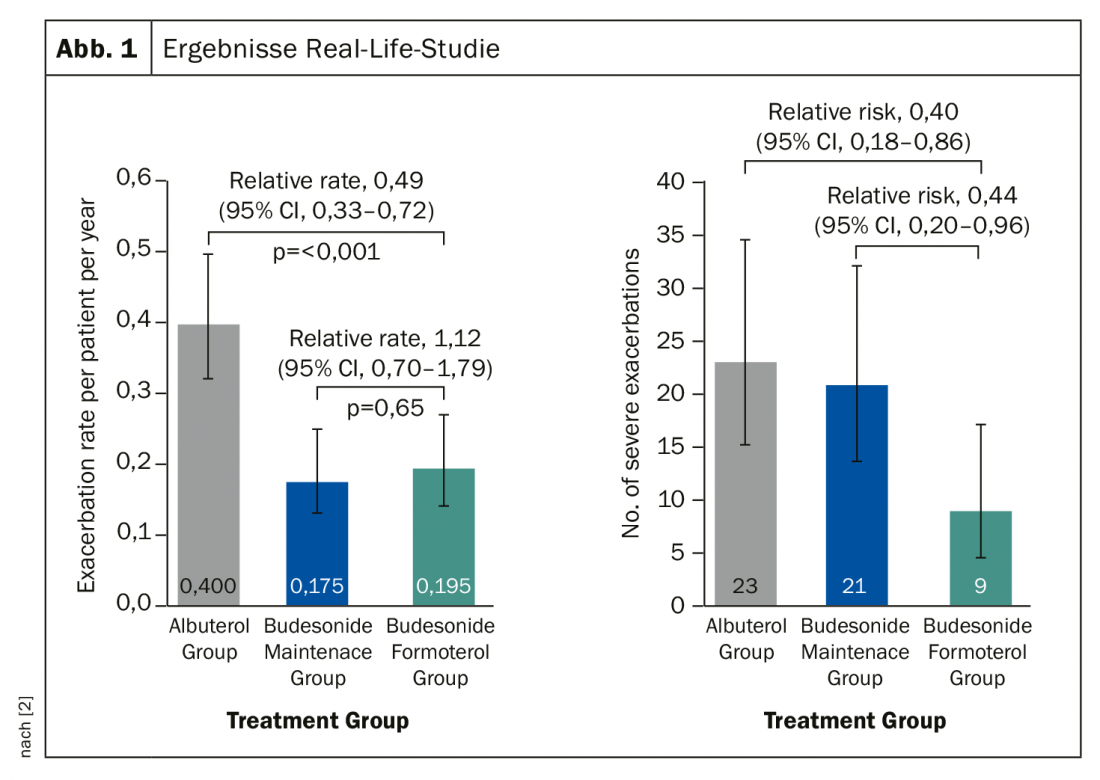
The primary test parameter was the annual asthma exacerbation rate. The result of this study again provided a clear message: with regard to all exacerbations, a steroid when needed proves to be just as effective in the long term in prevention as a steroid taken permanently. On symptom control alone, continuous therapy is marginally superior. Thus, ICS/formoterol on demand was as good as ICS on continuous therapy with SABA on demand. And the patients who took ICS/formoterol only when needed had a significantly lower risk of severe exacerbations (Fig. 1). “This is also obvious,” Prof. Buhl said: “When our patients get complaints, they take more demand medication. If they have ICS/formoterol as an on-demand medication, they automatically take more budesonide in the run-up to an exacerbation and thus automatically adjust their requirements. Patients on continuous therapy, on the other hand, can only take their ICS in the morning and evening.”
Also, asthmatic inflammation decreases with ICS/formoterol only when needed as effectively as with continuous therapy (as measured by nitric oxide in exhalate [FeNO, ppb]). Because, according to the expert, we are dealing with mild-grade diseases. This means that in continuous therapy there is a very low-threshold inflammation. This can obviously be well controlled whenever it flares up again by increasing the steroid dose for a short time.
ICS/formoterol on demand should therefore be considered equivalent to steroid continuous therapy and an alternative that accommodates the often intuitive behavior of patients. Such a therapy strategy has already been approved in Australia, New Zealand, Canada and many other countries. In Europe, the EMA has declined to approve ICS/formoterol preparations for such a strategy. Prof. Buhl is convinced that this will change in the future. For now, however, he told the full board, “you’re moving outside the permit with this station wagon.”
Nevertheless, GINA* has already responded: From the perspective of a population-based risk reduction strategy, the initiative recommends ICS/formoterol as an alternative strategy for patients older than 12 years.
Conclusion
- The ICS/formoterol combination is suitable as a controller and reliever for on-demand medication
- ICS dose with ICS/formoterol only when needed is only half that of ICS maintenance therapy plus SABA
- Less severe exacerbations on ICS/formoterol only as needed than on ICS maintenance therapy plus SABA.
- Comparable effect of ICS/formoterol only when needed and ICS maintenance therapy plus SABA on asthmatic inflammation (FeNO).
- Risk of exacerbation even in mild asthma reduced by approximately 50% with ICS/formoterol only when needed or ICS maintenance therapy
Source: Pneumo-Update 2019, Mainz (D)
* Global Initiative for Asthma
Literature:
- Reddel, et al: Eur Respir J 2019; 53(6): 1901046.
- Beasley R, et al: Eur Respir J 2016; 47: 981-984.
InFo PNEUMOLOGY & ALLERGOLOGY 2019; 1(3): 26-27 (published 9/12/19, ahead of print).