
An update on therapies currently available for plaque psoriasis. The introduction of biologics has changed the way patients with moderate to severe psoriasis are treated – with far-reaching implications for long-term quality of life.
Psoriasis is a chronic, inflammatory skin disease that affects approximately 2% of the Caucasian population [1]. Given the frequency of this dermatosis, it is important that primary care physicians are also regularly informed regarding new therapeutic options. Psoriasis can significantly reduce the quality of life of patients, especially in severe forms, with involvement of the hands including the nails, soles or joints (psoriatic arthritis). The diagnosis of psoriasis is usually made clinically. It is based on the typical efflorescences and their particular distribution. This article provides an update on the therapies currently available for plaque psoriasis (Figs. 1, 2).

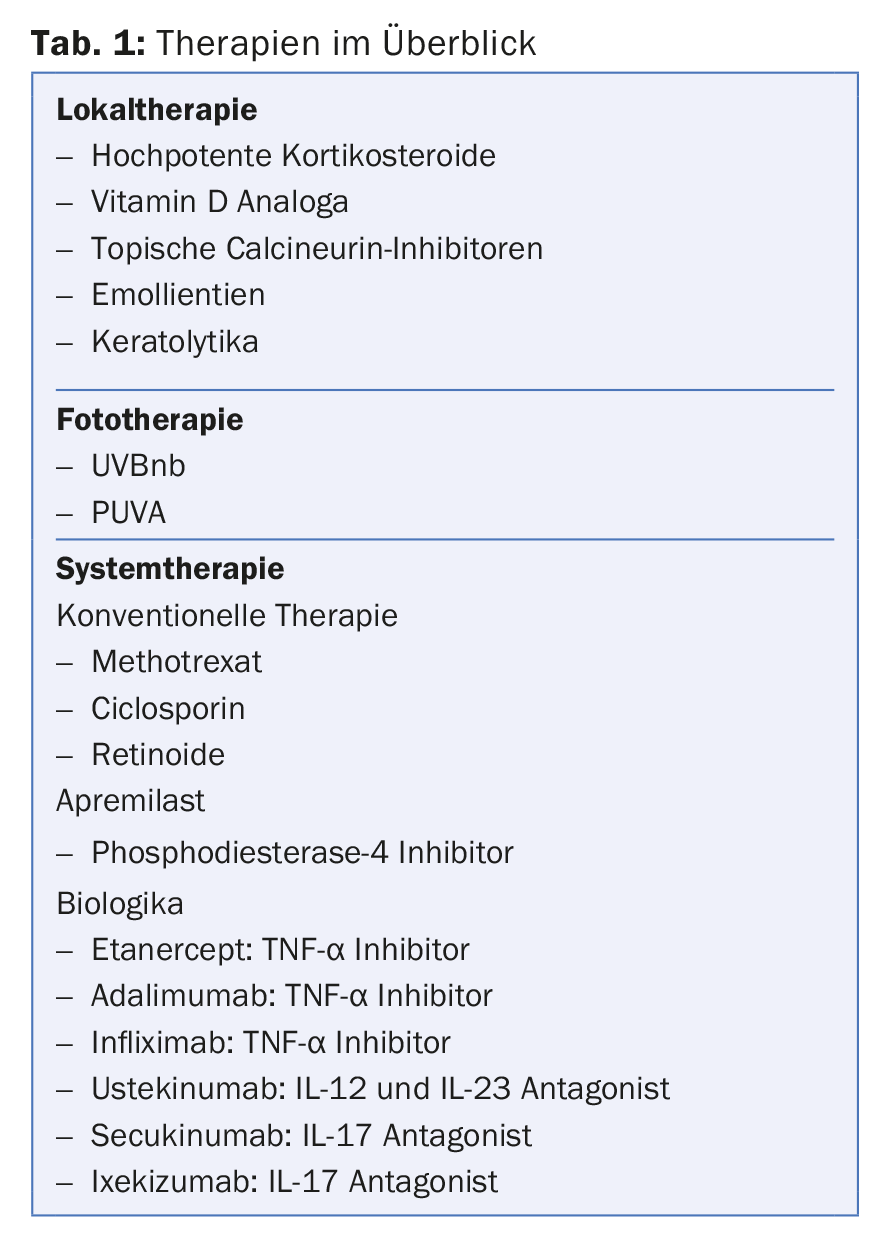
The introduction of biologics has changed the way patients with moderate to severe psoriasis are treated – with far-reaching implications for long-term quality of life. In the following, risk factors of psoriasis are discussed and local, phototherapy and finally systemic therapy are presented (Tab. 1).
Risk factors
While there is no doubt about the polygenetic cause of psoriasis, environment and lifestyle also play an important role. Before starting a therapy, it is important to illuminate all these aspects. Among the most important triggering factors are viral and bacterial infections, which can both induce an initial manifestation of psoriasis and worsen preexisting psoriasis. An example is guttate psoriasis secondary to angina caused by ss-hemolytic streptococci. In this case, the treatment of psoriasis includes antibiotic therapy.
It would be wrong to define psoriasis simply as a skin and joint disease. It is a systemic inflammatory disease that affects the entire organism. Cardiovascular events, diabetes mellitus, and obesity are known comorbidities of psoriasis. Weight reduction in obese patients often has a positive effect on psoriasis. Recent literature also shows an increased risk of white skin cancer, lymphoma, and lung cancer [2]. In addition, psoriatics suffer more often from depression and consumption of harmful substances (alcohol and nicotine). Climate also affects skin lesions with improvement in summer thanks to increased exposure to sunlight and humidity and deterioration in the cold and dry season. Not to be forgotten are the medications that can negatively affect psoriasis, such as lithium, beta-blockers, antimalarials, and interferon [3].
General considerations for therapy
To determine the optimal therapy it is necessary to consider the following factors:
- Type of psoriasis (plaque psoriasis, psoriatic arthritis, pustular psoriasis)
- Patient characteristics (age, pregnancy)
- Comorbidities (obesity, hepatopathy, cardiac or renal insufficiency).
- Severity of the disease
The PASI (Psoriasis Area and Severity Index), BSA (body surface area), and DLQI (Dermatology Life Quality Index) are used to define disease severity [1,4]. Taking all of these factors into account, and with certain exceptions (e.g., palmo-plantar psoriasis, nail involvement), local therapy or possibly phototherapy is preferred for mild psoriasis. Systemic treatment is more indicated for moderate to severe psoriasis [1].
The topical therapy
The backbone of local treatment of psoriasis is highly potent corticosteroids (e.g., mometasone and clobetasol propionate). These preparations are effective and applied to the lesions once daily, preferably in the evening [1]. After an induction period of about two weeks, the frequency of application is reduced to 1-3 times per week. Very important is the choice of galenics of the product: for very dry, scaly skin or in the genital area, an ointment is preferred. A cream or gel is used to treat acute and exudative lesions, while a lotion is more preferable for hairy areas. Excessive use of topical corticosteroids can lead to skin atrophy, telangiectasia, hypopigmentation, and perioral dermatitis, among others. Application to large body surfaces may also result in systemic side effects (e.g., iatrogenic Cushing’s syndrome).
Vitamin D derivatives (calcitriol and tacalcitol) are also effective for the topical treatment of psoriasis. They are applied 1-2 times a day. Local irritation may occur, which in turn is attenuated by the concomitant use of corticosteroids. For this reason, the combination of the two substances mentioned above is an excellent local treatment option and is also available as a corresponding product (calcipotriol and bethametasone). The topical use of calcineurin inhibitors (pimecrolimus, tacrolimus) for psoriasis is “off-label” and accordingly the costs are often not covered by health insurance. They have no antiproliferative effect on keratinocytes and their efficacy is lower than that of topical corticosteroids. The use of these preparations must be evaluated and reserved for special localizations (e.g., face) [1].
Psoriasis is characterized by skin barrier dysfunction and hyperproliferation of keratinocytes. Emollients and keratolytic substances such as salicylic acid 3-10% or urea 3-12% thus have a positive effect [1] and facilitate the penetration of corticosteroids. Avoid overly generous use of salicylic acid in children because of its potential nephrotoxicity and neurotoxicity, and combination with vitamin D because it is inactivated by salicylic acid.
The phototherapy
Phototherapy is an excellent therapy for psoriasis and can be combined with topical or systemic therapies (e.g., acitretin, psoralen) for resistant cases. The narrowband UVB spectrum (UVB TL01) is the most widely used. There is also PUVA (psoralen plus UVA), which combines phototherapy with photosensitizing agents. Here, a distinction is made between topical photochemotherapy (e.g. PUVA bath therapy) with e.g. the photosensitizer 8-methoxypsoralen and systemic photochemotherapy, in which case the photosensitizer is taken orally. The main limitations of phototherapy are logistical (usually three sessions per week for at least six weeks) and cutaneous carcinogenic potential, with UVB TL01 having a better safety profile than UVA light booths.
The systemic therapy
Approximately 20% of patients with plaque psoriasis require systemic therapy or phototherapy. The preparations available in Switzerland are methotrexate (MTX), acitretin, ciclosporin, apremilast and the biologics [4]. Since most of these drugs are immunosuppressants, clinical and laboratory tests are necessary beforehand. For most of these therapies it is necessary to exclude a latent chronic infectious disease (HIV, hepatitis B, hepatitis C, tuberculosis) as well as to check the vaccination record for completeness. Cancer that is not in remission is also a contraindication for the use of biologics.
Discussion of the well known conventional systemic therapy (methotrexate, acitretin and ciclosporin) will be omitted here in favor of introducing new molecules (apremilsate and biologics). To better assess the performance of these new drugs, the PASI75 is reported for each drug, expressing the percentage of patients who experienced at least a 75% reduction in their baseline PASI value over the course of treatment. A PASI75 of 43 at week 12 means that after three months of therapy, 43% of treated patients had an improvement in their psoriasis of at least 75% of their baseline score.
Apremilast (Otezla®) is a derivative of thalidomide and has been approved in Switzerland for more than two years. Apremilast has the advantages of easy therapy management (no mandatory regular laboratory analysis), a good safety profile, and oral administration. The “ESTEEM 1” studies showed a 75% reduction in PASI score at 16 weeks by 33% (versus 5% in patients receiving placebo) [5]. The most common side effects are nausea and diarrhea, each occurring in 14% to 16% of treated patients. The cost is about 1225 CHF per month, for example, compared to about 161 CHF per month of treatment with MTX with similar effect.
In recent years, biologics have radically changed the quality of life for patients with moderate to severe psoriasis. Indeed, conventional immunosuppressive therapies are characterized by a cumulative toxic effect on internal organs (MTX on the liver and ciclosporin on the kidneys). Thus, interruptions of systemic therapy were often necessary (rotation therapy). Biologics show no cumulative toxic risk and are prescribed in a continuous manner with reduction of troublesome exacerbations of dermatosis. These drugs have potentially severe side effects and, depending on the preparation, they may promote or cause severe infections (TB, hepatitis), demyelinating diseases, and severe heart failure [6].
Specific conditions must be met for reimbursement of these medications by health insurance: The patient must have moderate to severe psoriasis (PASI>10, BSA>10, or DLQI>10) and show no response to phototherapy or conventional systemic therapy. In Switzerland, the TNF-α inhibitors (etanercept, adalimumab and infliximab) and the monoclonal antibodies ustekinumab and secukinumab are available:
- Etanercept (Enbrel®): s.c. injection, which is usually prescribed in adults at a dose of 50 mg 1×/week. The onset of action is slower compared to the other TNF-α inhibitors, but etanercept can be used in children as young as six years of age. The PASI75 at 12 weeks is approximately 34% [7].
- Adalimumab (Humira®): human monoclonal antibody that binds to TNF-α. The dosage is 40 mg s.c. every two weeks. Therapeutic effects begin earlier than with etanercept, with a PASI75 at 12 weeks of approximately 53% [8].
- Infliximab (Remicade®): chimeric monoclonal antibody. Compared to the above-mentioned biologics, infliximab acts the fastest (effects already after 1-2 weeks). The dosage depends on body weight and therefore suitable for people with BMI>30, the disadvantage is the intravenous route of administration. The PASI75 at 10 weeks is approximately 75% [9].
- Ustekinumab (Stelara®): is injected only every 3 months in the maintenance phase and is an antagonist of interleukins-12 and 23. The ACCEPT study compared ustekinumab 45 mg (weeks 0 and 4) with etanercept 50 mg/2× per week. At week 12, the PASI75 was 68% (compared with 57% for etanercept) [10].
- Secukinumab (Cosentyx®): monoclonal antibody directed against interleukin 17A. This compound shows promising results also compared to other biologics with a PASI75 of 80% at week 12 . Side effects include frequent upper respiratory tract infections and Candida, staphylococcal and herpes infections. The recommended dose is 300 mg as a subcutaneous injection with starting doses at weeks 0, 1, 2, and 3, followed by monthly maintenance doses beginning at week 4. The monthly cost of this drug in the maintenance phase is approximately CHF 3085.
- Ixekizumab (Taltz®): the newest approved drug has only been available in Switzerland for a few months. As with secukinumab, this is an anti-IL-17 biologic. Both are characterized by the speed of the onset of action and thus a very rapid therapeutic success. In the UNCOVER-2 study, ixekizumab (80 mg subcutaneously every 2 weeks) produced a PASI75 in 50 percent of patients after only 4 weeks. After 12 weeks, 89.7% achieved a PASI75 with ixekizumab compared with 41.6% of patients in the etanercept group (50 mg 2× weekly). Side effects are similar to secukinumab [11].
In summary, in patients with mild psoriasis, topical therapy possibly with the addition of phototherapy is preferred, whereas in severe forms, systemic therapy is more indicated. As explained above, biologics are very effective for psoriasis. Their therapeutic effect is so superior to those of conventional therapies that the literature no longer speaks of PASI75, but of PASI90 (i.e. almost complete remission of psoriasis lesions)! However, these preparations have a wide range of possible side effects and their cost is much higher than those of conventional treatments. Careful consideration must therefore be given in advance to which drugs are appropriate for which patients.
Take-Home Messages
- Psoriasis therapy is based on severity, clinical type, and patient factors (such as age, pregnancy/breastfeeding, and comorbidities).
- In mild psoriasis, local therapy is effective and usually sufficient.
- The introduction of biologics has changed the way patients with moderate to severe psoriasis are treated.
Literature:
- Müller SM, et al: Therapy of plaque psoriasis. Schweiz Med Forum 2013; 13(06): 105-111.
- Chiesa Fuxench ZC, et al: The Risk of Cancer in Patients With Psoriasis: A Population-Based Cohort Study in the Health Improvement Network. JAMA Dermatol 2016; 152(3): 282-290.
- Takeshita J, et al: Psoriasis and comorbid diseases: Implications for management. Am Acad Dermatol. 2017; 76(3): 393-403.
- Kolios AGA, et al: Swiss S1 Guidelines on the Systemic Treatment of Psoriasis Vulgaris. Dermatology 2016; 232(4): 385-406.
- Papp K, et al: Apremilast, an oral phosphodiesterase 4 (PDE4) inhibitor, in patients with moderate to severe plaque psoriasis: Results of a phase III, randomized, controlled trial (Efficacy and Safety Trial Evaluating the Effects of Apremilast in Psoriasis [ESTEEM] 1). J Am Acad Dermatol. 2015;73(1): 37-49.
- Oussedik E, et al: The severe and acute complications of the biologics in psoriasis. G Ital Dermatol Venereol. 2017; 12 doi: 10.23736/S0392-0488.17.05750-9. [Epub ahead of print]
- Nguyen TU, Koo: Etanercept in the treatment of plaque psoriasis. Clin Cosmet Investig Dermatol. 2009; 2: 77-84.
- Mease PJ, et al: Adalimumab for long-term treatment of psoriatic arthritis: 2-year data from the Adalimumab Effectiveness in Psoriatic Arthritis Trial (ADEPT). Ann Rheum Dis. 2009; 68(5): 702-709.
- Leman JA, Burden AD: Treatment of severe psoriasis with infliximab. Ther Clin Risk Manag. 2008; 4(6): 1165-1176
- Young MS, et al.:The ACCEPT study: ustekinumab versus etanercept in moderate-to-severe psoriasis patients. Expert Rev Clin Immunol 2011; 7(1): 9-13.
- Leonardi CL, et al: Rapid improvements in health-related quality of life and itch with ixekizumab treatment in randomized phase 3 trials: results from UNCOVER-2 and UNCOVER-3. J Eur Acad Dermatol Venereol 2017; doi: 10.1111/jdv.14211 [Epub ahead of print].
DERMATOLOGIE PRAXIS 2017; 27(5): 8-12









