Experts recommend colorectal cancer screening in patients aged 50 and older. It is scientifically proven that structured preventive measures are associated with a reduction in mortality rates. This is due to the fact that colorectal tumors are readily treatable at an early stage.
Colorectal cancer is one of the most common cancers, mostly affecting people over the age of 50. Often the symptoms develop insidiously. Cancers of the colon, rectum and rectal area are grouped under the term “colorectal carcinoma”. If treated at an early stage, the chances of cure are good compared to other types of cancer. It is estimated that it takes about ten years for a benign polyp in the intestine to turn into a malignant tumor. Colorectal carcinomas manifest oligosymptomatically. The most common signs of an intestinal tumor include altered bowel habits and blood in the stool. Surgery, chemotherapy and radiation therapy are used for treatment.
Non-modifiable and modifiable risk factors
“In Switzerland, approximately 4500 new cases of colorectal carcinoma occur per year,” explains PD Emanuel Burri, MD, Head of Gastroenterology, Baselland Cantonal Hospital [1]. In connection with lifestyle factors and demographic developments, there has been an increase in the incidence of colorectal carcinomas in Western industrialized countries. Referring to WHO data, the incidence of colorectal cancer is predicted to increase by 50-60% by 2040 in the absence of measures, with a particularly high risk for those over 70 years of age [1]. “The biggest and most important risk factor is age,” the speaker explained. Among modifiable risk factors, obesity and nicotine use are among the most important triggers of colorectal cancer. Most colorectal tumors occur spontaneously, meaning that there is no family history of the disease. This means that even if there are no known tumors in the family, the speaker emphasizes that a diagnosis should be made. In Switzerland, the recommendation is that colonoscopy should be performed every 10 years, and an interval of two years is suggested for evidence of blood in the stool. However, in this country only 13% of all persons over 50 years of age take advantage of the opportunity to be screened for colorectal cancer, even though a new regulation on cost coverage by the mandatory health care insurance has been in force since 2013. This is too little, which is why several cantons have launched structured preventive measures.
Screening programs are associated with mortality reduction
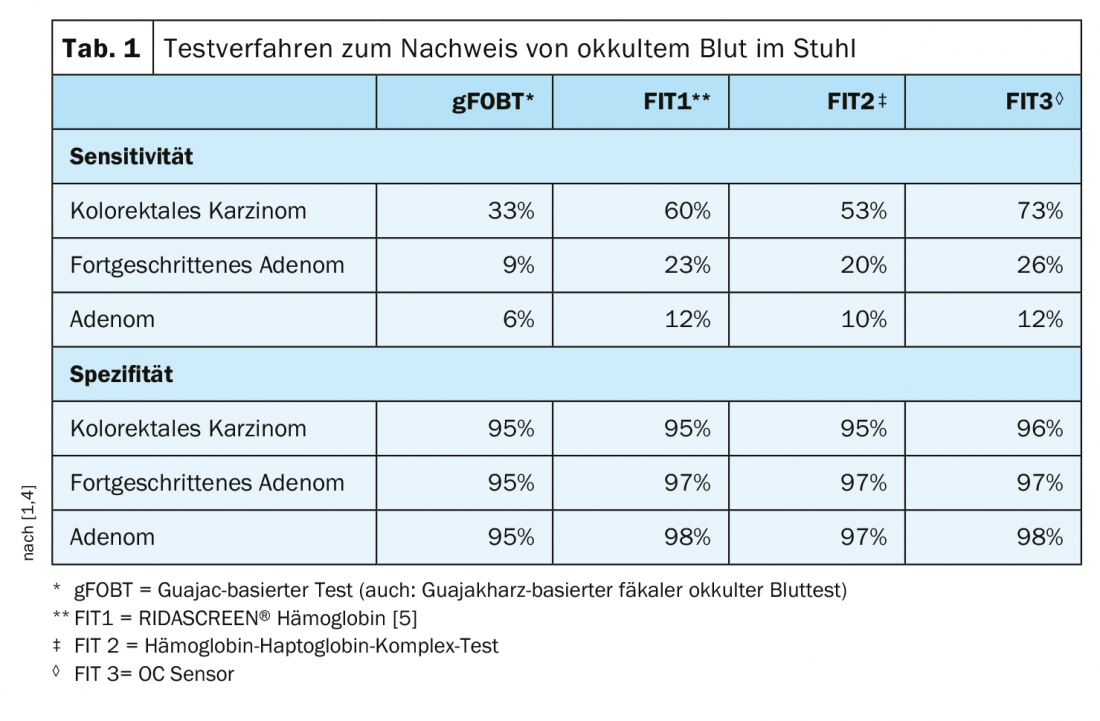
An overview of test procedures and their quality criteria can be seen in Table 1. Colonoscopy has high sensitivity for the detection of both carcinomas and adenomas and has a lower “number needed to screen.” Nowadays, it is also a procedure with few complications. The effect of implementing a structured screening program was investigated in the USA within the framework of the “Kayser Permanente Cohort”, which involved a sample of almost 1 million patients, according to the speaker [1]. The key message is that mortality rates in this cohort have been significantly reduced since the introduction of these stringent preventive measures [2]. This reflects the tactile fact that if tumors are diagnosed at an early stage, they can be treated well, Dr. Burri explains. The effect of the preventive measures was particularly high in the older population group, i.e. in the subpopulation with a higher tumor risk. In Switzerland, the Swiss Society of Gastroenterology has established quality criteria for the performance of screening colonoscopy [3].
Among other things, intestinal cleansing is one of the prerequisites for reliable results. “Only a clean bowel can be examined with good accuracy and safety for tumor screening,” the speaker explained.
The overall quality criteria for screening colonoscopy are as follows [1,3]:
- Number of examinations: at least 200 colonoscopies per year
- Bowel Preparation: Boston Bowel Preparation Score
- Complete colonoscopy at least 90% (target: 95%)
- Retraction time at least 6 min
- Adenoma Detection Rate (ADR)
- The perforation rate per examiner is less than 1/1000
- The bleeding rate after polyectomy is less than 1/100
- The documentation rate incl. Complications is 100%
There are also guidelines for follow-up polypectomy. Depending on the size, number, and histologic nature of the adenomas, follow-up every 3, 5, or 10 years is recommended, provided the estimated life expectancy is at least 10 years.
Source: FOMF Webup
Literature:
- Burri E: Colorectal cancer screening: evidence-based diagnostics. PD Dr. med. Emanuel Burri, Head of Gastroenterology, Cantonal Hospital Baselland. WebUp (video conference), 06.04.2020.
- Levin TR, et al: Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology 2018; 155(5): 1383-1391.e5.
- Swiss Society of Gastroenterology, https://sggssg.ch
- Brenner H, Tao S: Superior diagnostic performance of faecal immunochemical tests for haemoglobin in a head-to-head comparison with guaiac based faecal occult blood test among 2235 participants of screening colonoscopy. European Journal of Cancer 2013; 49(14): 3049-3054.
- R-Biopharm AG: https://clinical.r-biopharm.com/de/produkte/ridascreen-haemoglobin
HAUSARZT PRAXIS 2020; 15(5): 36-37 (published 8.5.20, ahead of print).









