
In addition to expertise, patients with hair loss need advice above all. Dermatologist Myriam Wyss Fopp, MD, offers this in her hair consultation. She also led the Zurich study site as part of an international 5-year multicenter study with finasteride. In this interview, Dr. Wyss gives a brief insight into her work.
Dr. Wyss, how many men and women do you see in the hair consultation?
Dr. Wyss: An estimated 90% women and 10% men. Trichological patients make up a large part of my consultation. At the beginning of the finasteride era in 1997, the sex ratio was approximately 50:50. The media presence of finasteride during the launch led to many men becoming aware of the new treatment option or being informed by their wives. Today, in my observation, fewer men than back then know that drug treatment is available.
Do you take a gender-specific approach to diagnosis, therapy and counseling?
Dr. Wyss: Yes, in men I perform a clinical examination with scalp inspection, dermoscopy and standardized photographs. If the diagnosis of androgenetic alopecia is unequivocal, I do not perform further diagnostics. If a man decides to undergo finasteride treatment, I determine the PSA level beforehand, as this drops as a result of the treatment.
In cases with advanced androgenetic alopecia, I personally think it makes more sense to cut the hair very short instead of starting drug therapy. I communicate this to the patient accordingly. When an honest opinion is conveyed along with a compliment, e.g. for an attractive head shape, it is easier for the patient to accept and is usually appreciated.
For the ladies, I arrange for a more comprehensive workup: clinical examination, dermoscopy, photo documentation, trichogram and laboratory analysis.
I also ask specifically about androgenization symptoms. In women, there are often several cumulative factors, e.g., androgenetic alopecia may first be unmasked by iron deficiency or postpartum effluvium.
Another tip for photo documentation: Make sure the patients appear with freshly dyed hair. A gray approach distorts the photo image.
What do patients often do wrong?
Dr. Wyss: A few things! Many think that hair loss is a diagnosis, not a symptom, which can have many causes. The first port of call for hair loss is often the hairdresser, the pharmacy or the drugstore. There, the level of knowledge is very variable. Without a precise diagnosis, reconstructive preparations and tinctures are used.
Often a lot of time and also money is lost until a well-founded clarification of the cause takes place. Unfortunately, there is also a trend toward pseudoscientific studies such as mineral analysis….
Then there are also very practical errors and traditional misconceptions. For example, that frequent shampooing promotes hair loss. Instead of washing the hair frequently, the hair is then strained with hairstyle-enhancing measures such as toupeeing. Thus, in addition to androgenetic alopecia, exogenous hair shaft damage follows. Another stumbling block in treatment: hair patients read the package insert too carefully.
Seriously? What do you mean?
Dr. Wyss: Hair patients are often very meticulous. Part of my job is to debunk the fears fueled by studying the potential side effects. I have had a few patients return a minoxidil solution because it was such a dangerous drug or because it was impossible for the patient to keep the 12-hour rhythm exactly.
Several patients also discontinued treatment with minoxidil when they reached 65 years of age because they had interpreted the patient information in this way.
What do you advise patients who have already “tried everything”?
Dr. Wyss: For women with high levels of suffering who have already tried everything, I also inform them about the possibility of a computer-assisted deep scalp massage, which increases blood flow. Patients are informed that this is not a method with scientific proof of efficacy. Theoretically, an effect e.g. via the “Vascular Endothelial Growth”-Factor (VEGF) is well conceivable.
Another interesting method is the injection of autologous platelet-rich plasma (PRP), which we also use in skin rejuvenation treatments. There is experimental evidence that PRP induces proliferation of cells of the dermal papilla as well as exerts an anti-apoptotic effect on the same cells. However, long-term experience has yet to be gained. Patients who decide to undergo treatment need to know this.
Injection of PRP and computer-assisted vacuum treatment of the scalp provide an additional treatment option for women with androgenetic alopecia in whom established therapy is limited to minoxidil.
In your opinion, how useful is the intake of vitamins and trace elements?
Since these preparations are often taken by the patients as the first therapy at random, unfortunately sometimes a lot of time passes before the cause of the effluvium is clarified. I have even had male patients with clear androgenetic alopecia who conscientiously swallowed build-up preparations. It is logical that hair building preparations cannot bring success in case of iron deficiency or a thyroid disorder. Personally, I recommend them in cases of convalescence or seasonal effluvium, for example, when the causes have been clarified.
When do you use finasteride, when minoxidil?
If the patients are over 18 years old and the diagnosis of androgenetic alopecia is established, I provide information about both treatment methods and their chances of success. In most cases, the patients then know exactly which treatment they prefer. It is, after all, a lifestyle treatment. Occasionally, we combine both medications. An additive effect of minoxidil and finasteride was demonstrated in macaques.
What should you look for in shampoos?
In the hair consultation, we pay attention to whether a scalp dermatosis is present in addition to the effluvium, e.g. seborrheic eczema. If so, antifungal shampoos are useful. If the hair is washed frequently, e.g. daily, a mild shampoo should be used. Patients with oily scalp or seborrheic dermatitis need to know that frequent hair washing is not harmful. For irritated scalp, mild conditioning shampoos containing witch hazel extract or heart seed (Cardiospermum) may also be recommended, which have an anti-irritant effect.
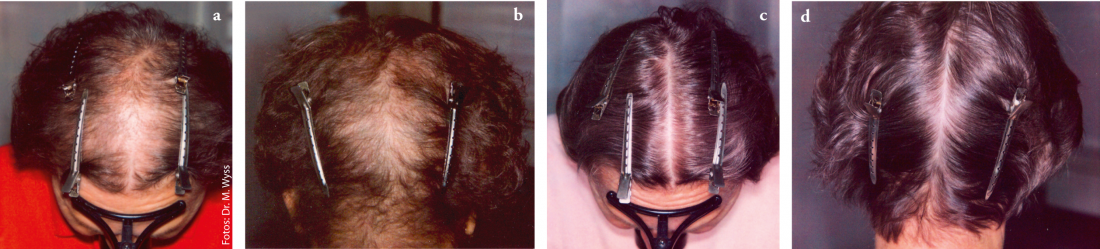
Fig. 1 a-d: Patient with alopecia diffusa in thyroid disorder, before (a, b) and after (c, d) six months of treatment.
What makes a hair consultation successful from your point of view?
Dr. Wyss: Empathy is what makes it. Hair loss often causes stress and anxiety. Time must be taken to discuss even seemingly trivial issues in detail, e.g., the use of topical therapeutics, hair care, etc. Trichological patients in particular want to be guided safely and be able to adhere to a precise, well-structured treatment plan. The therapy concept is to be coordinated individually. In my opinion, it is essential that the success of treatment is objectively recorded, preferably by means of standardized photographic documentation. This motivates both the patients and the treating physician.
Interview: Susanne Schelosky, M.D.









