
Anxiety disorders, along with depression, are among the most common disorders in the field of psychiatry. While fear is an emotional response to a specific threat, anxiety is an anticipation of future threats. A wide range of anxiety disorders are now distinguished – with implications for treatment regimens.
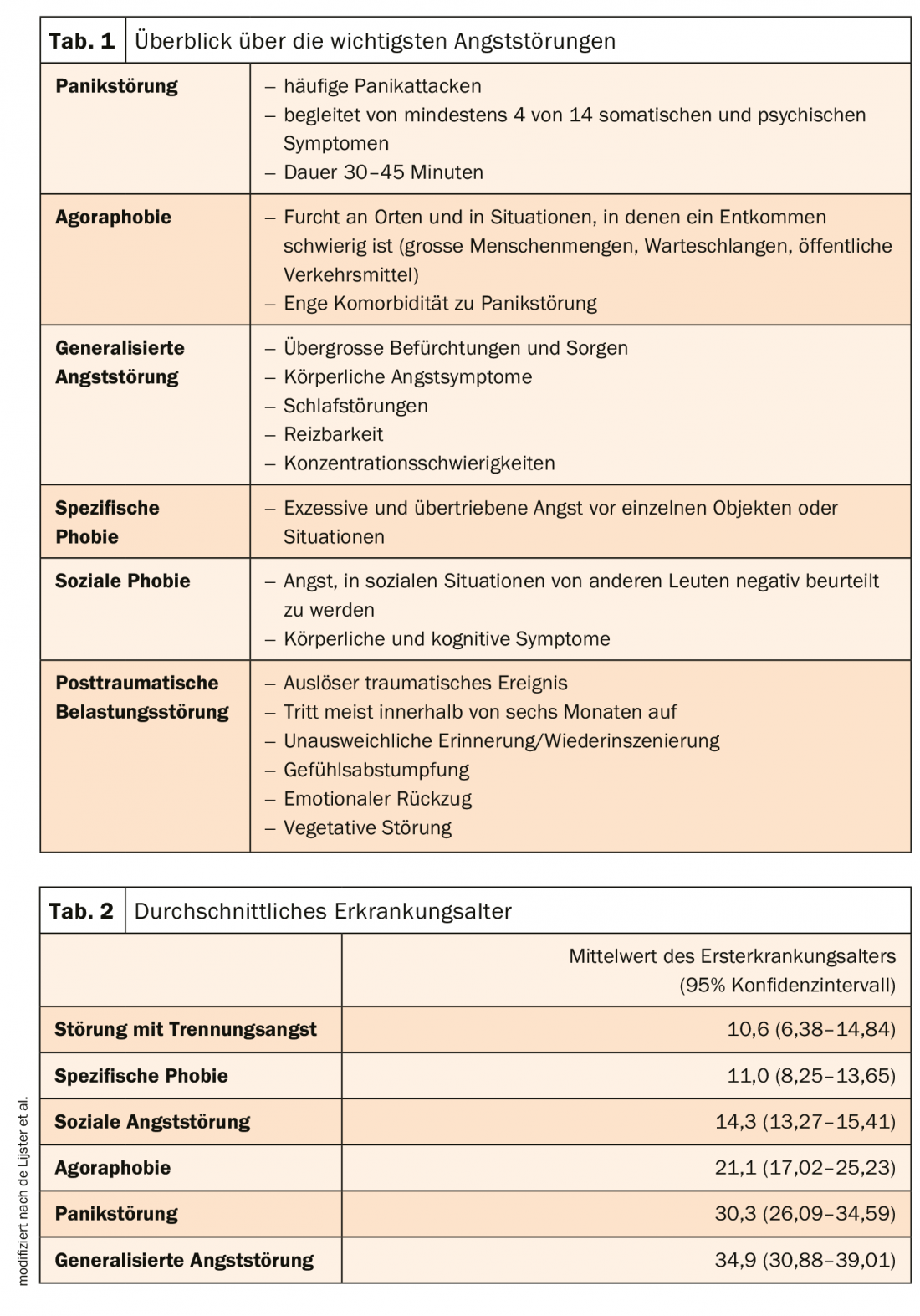
Actually, evolution meant well. Our “fight-or-flight” response allows us to adapt quickly to dangerous situations. However, if the concrete threat from external factors is missing and the anxiety occurs nevertheless, the picture of an anxiety disorder is given. Anxiety symptoms manifest themselves primarily in shortness of breath, palpitations, agitation, muscle tension, tremors, and a dry mouth. These physiological responses prepare the body for fight or flight. The clinical picture is differentiated into separation anxiety disorder, selective mutism, specific phobia, social anxiety disorder, panic disorder, agoraphobia, generalized anxiety disorder and post-traumatic stress disorder (Tab. 1) . They differ in both onset and course of illness (Tab. 2).
The diagnosis is based on the differentiation between symptom, syndrome and diagnosis level. At the symptom level, the focus is primarily on physical complaints. In addition, avoidance behavior and worry or social behavior strategies are recorded. At the syndrome level, it is mainly the severity that is assessed. Self-assessment and third-party assessment scales are used for this purpose. Initial indications of the diagnosis are usually already apparent in spontaneous descriptions of the complaints in the free clinical interview. However, since this is often not reliable enough, standardized interviews should be used in the further course. In addition, the possibility of comorbid conditions such as depression, psychotropic substance disorders, somatoform disorders, or other anxiety disorders should be closely examined.
Comprehensive help for self-help
The gold standard for the treatment of anxiety disorders is a combination of cognitive behavioral therapy (CBT) and pharmacologic interventions. However, psychotherapy is often not available in a timely manner. Suggestions for self-help should be given here to bridge the waiting time. Recently, the first steps have been taken in the direction of Internet therapy to help sufferers cope with their psychological problems. Meanwhile, offerings such as Internet-based cognitive-behavioral therapy or guided self-help approaches exist. However, studies have demonstrated that the combination of CT and drug therapy is often superior to the respective monotherapy. Therefore, a comprehensive treatment regimen tailored to the individual should be developed.
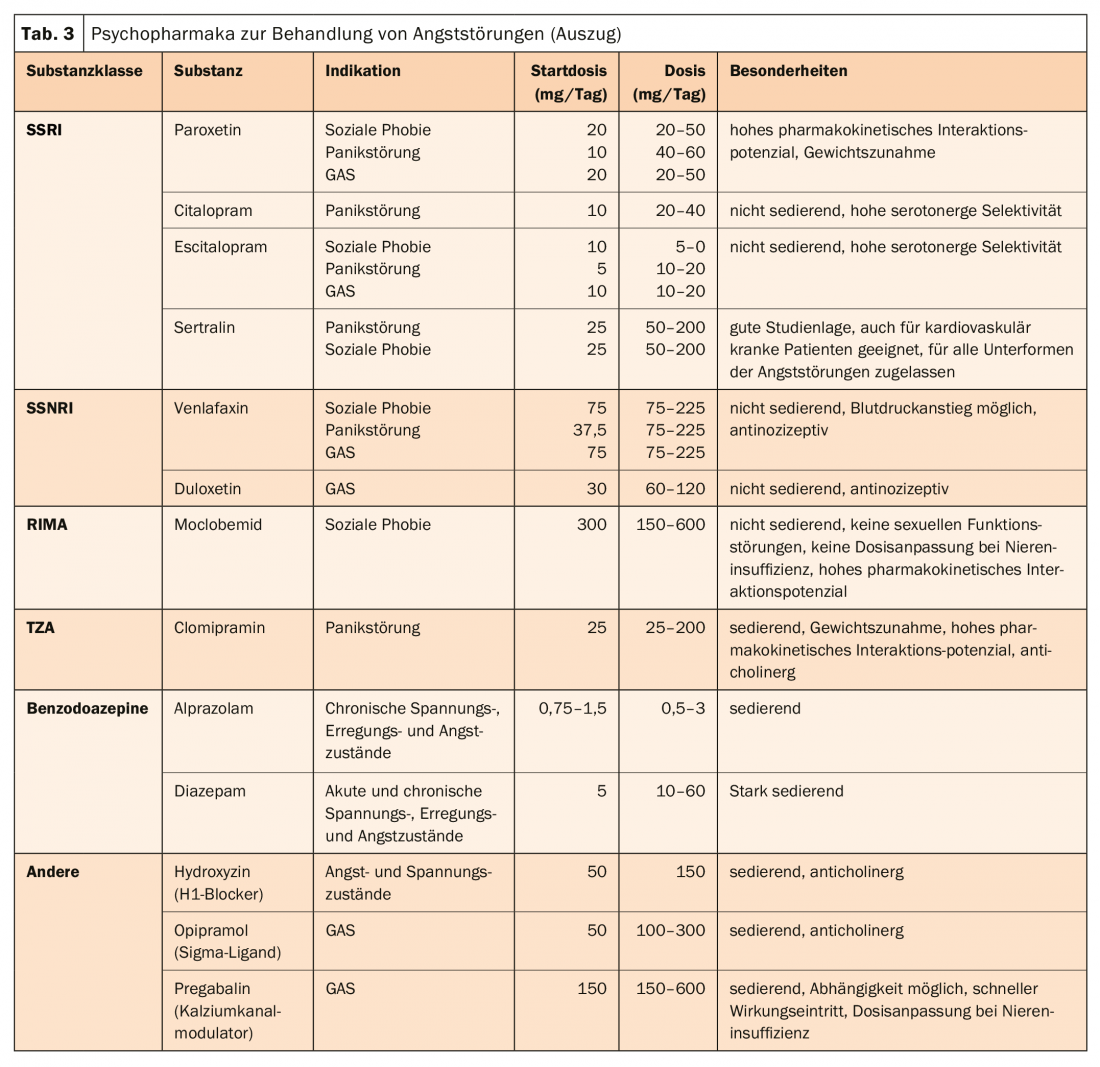
Basically, pharmacological therapy of anxiety disorders is divided into three phases: acute therapy, maintenance therapy, and prophylactic therapy. A number of substances from different substance classes are available for drug treatment (tab. 3) . The drugs of first choice are primarily selective serotonin reuptake inhibitors (SSRIs) and increasingly also selective serotonin-norepinephrine reuptake inhibitors (SSNRIs). However, their effect unfolds only after 2 to 6 weeks. Therefore, comedication with benzodiazepines may be useful at the beginning. In this way, the acute symptoms can be cupped and the effect latency can be bridged. However, they should not be given for more than one to two weeks.
Further reading:
- Volz HP, Stieglitz RD: Anxiety disorders-diagnosis, psycho- and pharmacotherapy. DNP – The Neurologist & Psychiatrist 2019. 20(6): 90-99.
- De Lijster JM, et al: The age of onset of anxiety disorders: a meta-analysis. Can J Psychiatry 2017; 62(4): 237-246.
- %C3%(letzter Zugriff am 27.03.2020)
- https://oegpb.at/wp-content/uploads/2018/12/Konsensus_Angststoerungen_29_10_2018.pdf (last accessed on 27.03.2020)
- www.rosenfluh.ch/media/arsmedici/2014/14-15/Pharmakotherapie_bei_Angststorungen.pdf (last accessed on 27.03.2020)
InFo NEUROLOGY & PSYCHIATRY 2020; 18(3): 44-46.









