
Pancreas transplantation is a standard treatment option for patients with type 1 diabetes and concomitant higher-grade diabetic nephropathy. Pancreas transplantation offers the chance of permanent insulin freedom, a reduction in concomitant diabetic diseases and a significant improvement in quality of life. From a surgical point of view, pancreas transplantation has become very safe. The parameters of donor conditioning, organ retrieval, graft assessment, and back-table preparation that affect postoperative complication rates have an impact on success. Pancreas transplantation continues to have the highest complication rate of all solid organ transplants. On the other hand, patients after pancreas-kidney transplantation have an extended life expectancy of about 15 years compared to type 1 diabetics without transplantation.
Glycemic control by insulin injections is often unsatisfactory and associated with multiple long-term complications such as retino-, neuro-, vasculo- and nephropathies [1]. Mortality in type 1 diabetics is high at 13% after 20 years [2]. In the case of additional terminal renal failure, life expectancy deteriorates dramatically [3].
Pancreas transplantation mostly in combination with kidney transplantation
Pancreas transplantation is the only therapy that leads to long-term normoglycemia and normalization of HbA1c levels in type 1 diabetic patients [4]. Combined pancreas-kidney transplantation is among the established therapies for type 1 diabetics with (pre)end-stage renal failure. In Europe, a majority (89%) of pancreas transplants are performed in combination with kidney transplantation. Improvements in surgical techniques, new immunosuppressive drugs, and better management of postoperative complications have improved 1-year survival of patients and pancreas graft after combined transplantation from 67% and 21% (1980) to 95% today resp. 85% improved.
Since the first successful combined pancreas-kidney transplantation in 1966 by Lillehei and Kelly (Minnesota, USA) [5], numerous techniques of pancreas transplantation have subsequently been described due to complications. Today, the entire pancreas is transplanted with the short, blind-occluded duodenum [6]. The donor duodenum can be anastomosed to either the urinary bladder (bladder drainage) or the upper jejunum (small bowel drainage). Until the mid-1990s, bladder drainage was the main procedure performed. This procedure allowed graft monitoring by determination of amylase and lipase in urine, but was characterized by the occurrence of severe metabolic acidosis (bicarbonate loss) and urologic problems (urinary bladder and urethral infections) and has since been largely abandoned [4]. Today, most transplant centers drain pancreatic juice into the anastomosed jejunum (small bowel drainage technique), usually in combination with kidney from the same donor. At the same time, transplantation remains prone to complications (35-80%) [7]. In Switzerland, 25-30 pancreas transplants are performed annually at the University Hospitals of Geneva and Zurich,
usually in combination with a kidney transplant.
Indication
The classic indication for simultaneous pancreas-kidney transplantation is the juvenile type 1 diabetic with negative C-peptide and (pre)terminal renal failure (Tables 1 and 2) . However, in recent years, patients with creatinine clearance above 40 ml/min have been increasingly evaluated for combination transplantation and have been transplanted before requiring dialysis. This preemptive transplantation leads to a reduction in perioperative mortality and significantly improves long-term patient survival [8]. The main purpose of pancreas transplantation is to replace missing or deficient insulin production.
The indication for isolated pancreas transplantation can only be given in patients in whom diabetes remains extremely unstable despite all conservative therapeutic measures. In these rare cases, renal function should be unaffected or minimally affected because of the expected nephrotoxicity of immunosuppressive therapy [9]. Patients with type 2 diabetes mellitus remain exceptional cases, accounting for 1-8% of pancreas transplants worldwide. Pancreas transplantation in type 2 diabetics should be performed only in exceptional cases after critical recipient selection (Table 3).
Organ removal
Pancreas retrieval is usually performed as part of a multiorgan donation via a median laparotomy from the xyphoid to the symphysis with or without sternotomy. After standardized dissection, the visceral organs are perfused with cold preservation solution via an aortic or iliac perfusion tube. In addition, the organs are cooled topically with crushed ice and cold NaCl solution. The pancreas and liver can be removed en bloc or separately.
Back table reconstruction
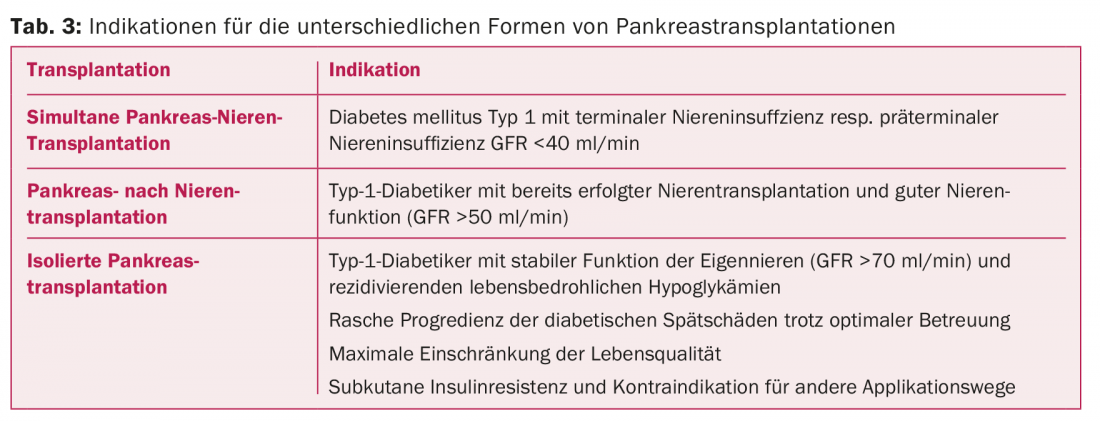
Backtable preparation should be performed by the transplanting surgeon. A donor Y-graft consisting of the common iliac artery and its branching into the internal and external iliac arteries is used as standard for reconstruction of an arterial conduit by connecting the internal iliac artery to the lienal artery and the external iliac artery to the superior mesenteric artery as end-to-end anastomoses (Fig. 1).
Combined pancreas-kidney transplantation
Transplantation of the pancreas is performed heterotopically in the abdomen (Fig. 2). Primarily, the pancreas is transplanted and the right pelvic axis is preferred for revascularization for anatomical reasons. Venous diversion of the pancreas is performed first; it may be systemic-venous to the external iliac vein or inferior vena cava, or portal-venous to the inferior mesenteric vein. Systemic venous drainage is the standard technique at most transplant centers despite postoperative peripheral hyperinsulinism [10], although some centers already prefer endocrine physiologic drainage into the portal circulation. The arterial anastomosis consists of the donor iliac, which is ideally sutured end-to-side to the recipient’s A. Iliaca externa of the recipient in continuous suture or single button suture technique.
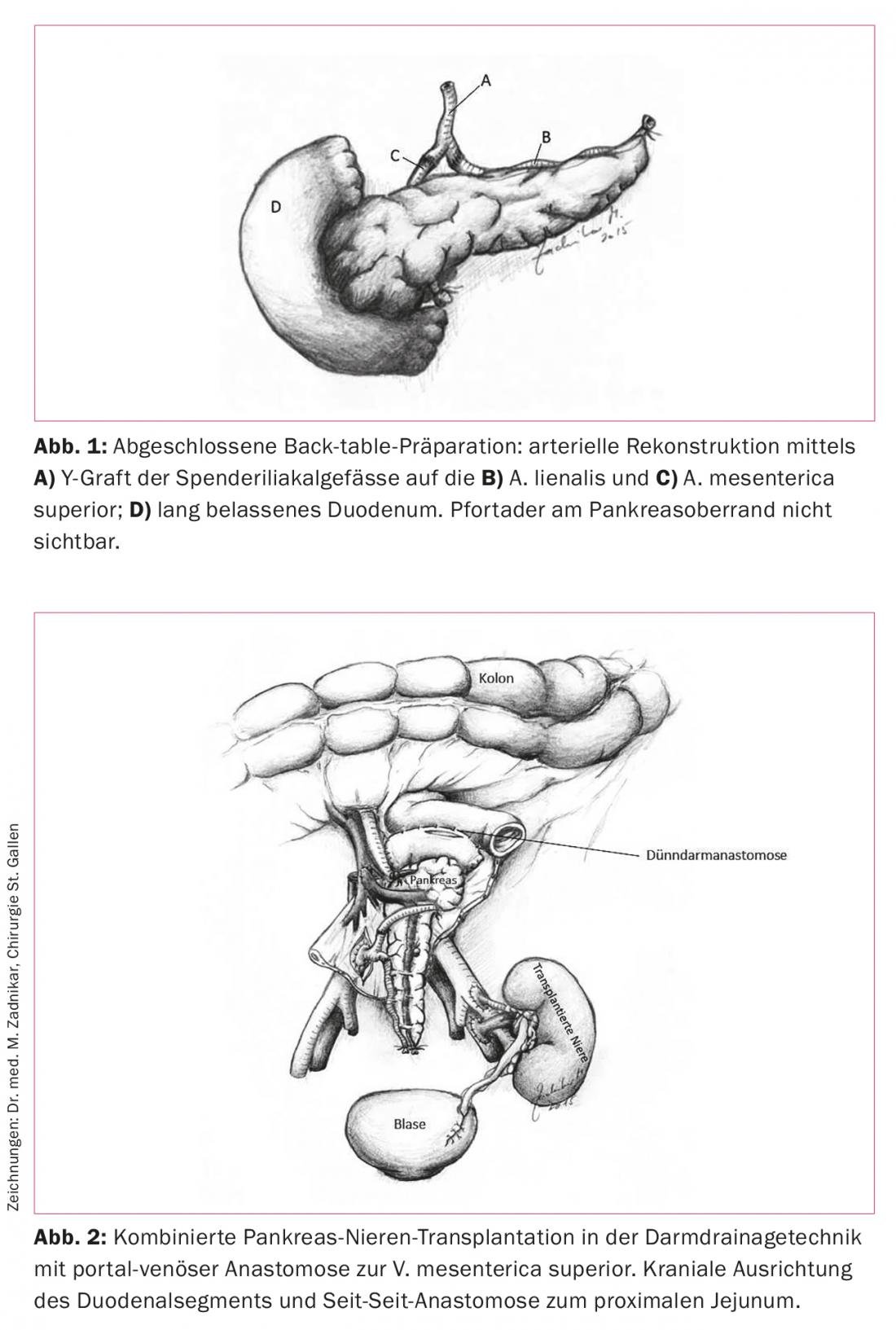
For reperfusion, the venous limb is opened first. Hemorrhage into the pancreatic capsule should be avoided at all costs. Subsequently, the arterial limb is released. After successful hemostasis, exocrine drainage is performed. This is done with the small bowel drainage technique approximately 50 cm aboral to the Treitz flexure using side-to-side duodenojejunostomy. The small bowel drainage technique later allows endoscopic graft evaluation by obtaining transduodenal tissue samples.
Survival rates
The 5- and 10-year survival rates of patients with simultaneous pancreas-kidney transplantation are 87 and 70%, respectively [11]. Pancreas graft survival rates after combined transplantation are 86% at one year and still 53% at ten years. In this context, renal function is 95% preserved after one year >and 60% preserved after ten years [12]. The lower survival rate of pancreata is due to the early postoperative complications such as thrombosis, pancreatic fistula, and infections [13].
One study analyzed the mortality risk of 13 467 diabetic patients after pancreas-kidney transplantation, kidney transplantation, and dialysis therapy during ten years. Compared to kidney transplantation alone, significantly better survival after ten years was shown after pancreas-kidney transplantation (67 vs. 46%, p<0.001). Pancreas-kidney transplant recipients had the longest expected survival (23.4 years), compared with 13 years of patients after kidney transplant and eight years of patients on the transplant waiting list and dialysis [14].
Quality of life after pancreas transplantation
Pancreas transplantation can improve quality of life by eliminating diabetes-associated complications (hypo/hyperglycemia, metabolic derailments, insulin dependence, daily blood glucose monitoring, dietary restrictions) [14]. Several studies show a significant improvement in quality of life after transplantation compared with pretransplantation studies [15].
Glucose control and impact on late diabetic complications.
Most patients achieve complete, short- and long-term insulin independence after pancreas transplantation has been performed. Control is significantly better than in patients with insulin pumps or who have undergone islet cell transplantation [16]. 15 years after successful pancreas transplantation, Mora et al. show that there was no significant difference in transplanted patients regarding HbA1c value in the first year after transplantation and HbA1c value in the last year before study inclusion (4.68 vs. 4.76%, p>0.05) [17]. The impact of pancreas transplantation on late diabetic complications such as retinopathy is controversial but mostly favorable [18]. Persistent normoglycemia may improve nerve function even in advanced polyneuropathy. Existing macroangiopathy is not improved by pancreas transplantation. The prevalences of cerebrovascular disease and PAVK five years after pancreas transplantation are 31% and 41%, respectively. Ten years after transplantation, prevalences increased discretely to 41% and 50%, respectively [19].
Transplant centers in Switzerland
Diabetic patients with advanced renal insufficiency (creatinine clearance ≤25 ml/min) can be assigned for consultation to one of the six kidney transplant centers in Switzerland (Basel, Bern, Geneva, Lausanne, St. Gallen, Zurich). These refer potential patients to the two pancreas transplant centers in Geneva and Zurich. The waiting time for a combined pancreas-kidney transplant is three to twelve months.
Literature:
- Lipshutz GS, et al: Pancreas-kidney and pancreas transplantation for the treatment of diabetes mellitus. Endocrinol Metab Clin North Am 2007; 36(4): 1015-1038.
- Stadler M, et al: Increased plasma amylin in type 1 diabetic patients after kidney and pancreas transplantation: A sign of impaired beta-cell function? Diabetes Care 2006; 29(5): 1031-1038.
- Fourtounas C: Transplant options for patients with type 2 diabetes and chronic kidney disease. World J Transplant 2014; 24(2): 102-110.
- Sollinger HW, et al: One thousand simultaneous pancreas-kidney transplants at a single center with 22-year follow-up. Ann Surg 2009; 250(4): 618-630.
- Kelly WD, et al: Allograft transplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967; 61: 827-837.
- Nghiem DD, et al:Transplantation with urinary drainage of pancreatic secretions. Am J Surg 1987; 153: 405-406.
- Stratta RJ, et al: A prospective comparison of simultaneous kidney-pancreas transplantation with systemic-enteric versus portal-enteric drainage. Ann Surg 2001; 233(6): 740-751.
- Morath C, et al: Metabolic control improves long-term renal allograft and patient survival in type 1 diabetes. J Am Soc Nephrol 2008; 19(8): 1557-1563.
- Ming CS, et al: Progress in pancreas transplantation and combined pancreas-kidney transplantation. Hepatobiliary Pancreat Dis Int 2007; 6(1): 17-23.
- Gruessner AC: 2011 update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the International Pancreas Transplant Registry (IPTR). Rev Diabet Stud 2011; 8(1): 6-16.
- McCullough KP, et al: Kidney and pancreas transplantation in the United States, 1998-2007: access for patients with diabetes and end-stage renal disease. Am J Transplant 2009; 9: 894-906.
- Ziaja J, et al: Does simultaneously transplanted pancreas improve long-term outcome of kidney transplantation in type 1 diabetic recipients? Transplant Proc 2011; 43(8): 3097-3101.
- Ojo AO, et al: Long-term benefit of kidney-pancreas transplants in type 1 diabetics. Transplant Proc 2001; 33(1-2): 1670-1672.
- Martins LS, et al: Health-related quality of life may improve after transplantation in pancreas-kidney recipients. Clin Transplant 2015; 29(3): 242-251.
- Smith GC, et al: Prospective quality-of-life monitoring of simultaneous pancreas and kidney transplant recipients using the 36-item short form health survey. Am J Kidney Dis 2010; 55(4): 698-707.
- Gerber PA, et al: Simultaneous islet-kidney vs pancreas-kidney transplantation in type 1 diabetes mellitus: a 5 year single centre follow-up. Diabetologia 2008; 51(1): 110-119.
- Mora M, et al: Pancreas and kidney transplantation: long-term endocrine function. Clin Transplant 2010; 24(6): E236-240.
- Pearce IA, et al: Stabilisation of diabetic retinopathy following simultaneous pancreas and kidney transplant. Br J Ophthalmol 2000; 84(7): 736-740.
- Biesenbach G, et al: Progression of macrovascular diseases is reduced in type 1 diabetic patients after more than 5 years successful combined pancreas-kidney transplantation in comparison to kidney transplantation alone. Transpl Int 2005; 18(9): 1054-1060.
CARDIOVASC 2015; 14(4): 10-13









