
Although many hypertensive patients perform regular blood pressure measurements at home, a large proportion of these patients – 51% in the SWISSHYPE study published in 2011 [1] – are inadequately treated or have a low blood pressure. does not reach the target blood pressure values. This is due on the one hand to a lack of compliance and adherence on the part of many patients, but often also to a therapy that is not optimally developed.
A team from the Institute of Family Medicine in Zurich has shown that blood pressure can be reduced with the help of a very simple and inexpensive intervention, namely the ab-
The results of the blood pressure test are impressive (syst. -14 mmHg, diast. -8 mmHg) [2, 3]. This is achieved on the one hand by increasing compliance and adherence and on the other hand by improving awareness on the part of both patients and physicians.
In practice, 24-hour blood pressure measurement is a cost-effective and time-efficient measure for diagnosing patients with high blood pressure. NICE guidelines recommend that all patients with a blood pressure >140/90 mmHg should have one performed first [4]. If the mean blood pressure in this measurement is 135-150/85-95 mmHg, it is recommended that only lifestyle measures be taken initially in patients with no end-organ damage and no increased cardiovascular risk (this can be determined using the AGLA risk calculator, for example, www.agla.ch). If the patient already has end-organ damage and/or an increased cardiovascular risk or if the values are >150/95 mmHg, drug treatment should be started in addition to lifestyle measures [4]. At the SGIM congress in Basel, Thilo Burkhard, MD, Basel, recommended that younger patients (<55 years) should always be started primarily with an angiotensin receptor blocker (ARB) or an ACE inhibitor and older patients with a calcium antagonist(Fig. 1) [4].
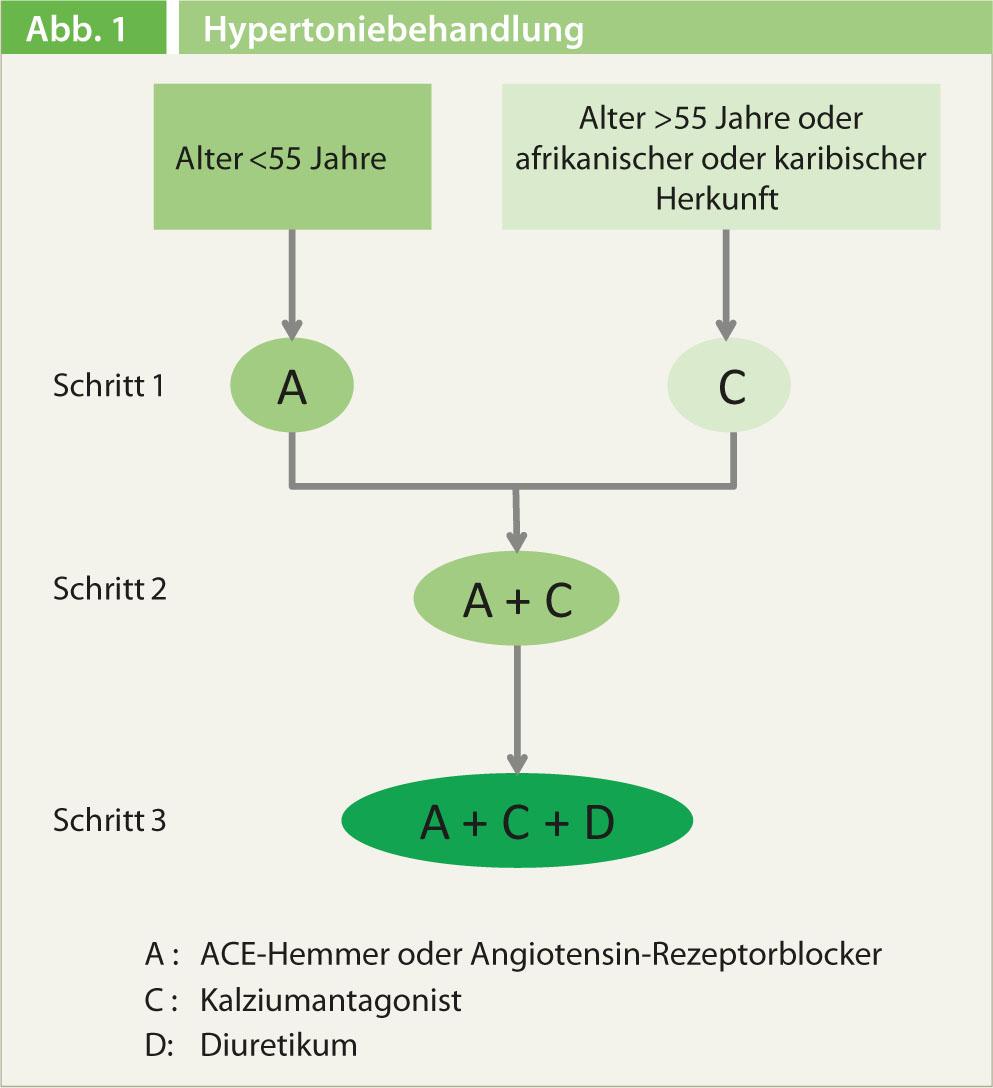
If monotherapy is not sufficient, ARB resp. ACE inhibitors and calcium antagonists are combined and only in a third step, if necessary, a diuretic is added [4]. According to Dr. Burkhard, most patients require combination therapy to achieve target blood pressure levels on a sustained basis. He therefore recommended that in patients with grade 2 hypertension or in the presence of end-organ damage – in addition to the lifestyle measures that always belong! – to consider a combination therapy already initially. Especially in patients who still need to take additional medications, fixed-dose combination preparations contribute to a significant improvement in adherence.
Source: “Hypertension Treatment in Family Practice – Good, but can it be better?” Satellite Symposium of A. Menarini AG, SGIM Congress, May 29-31, 2013, Basel.
Literature:
- Brenner R, et al: Swiss Med Wkly 2011; 141: w13169.
- Steurer-Stey C, et al: Trials 2010; 11: 38.
- Rosemann T: Results of the CoCo study. Paper presented at the SGIM Annual Meeting 2013.
- NICE: CG127, 2011. http://guidance.nice.org.uk/CG127









