
Apophysitis calcanei is an inflammation of the bony attachment of the Achilles tendon. It is most common in growing children and adolescents and is associated with swelling, redness and pain of the calcaneus. The apophysis is connected to the bone by cartilage tissue during the growth phase. At this point, irritation often occurs in the area of the Achilles tendon insertion due to overloading.
As the last articles on movement- and load-dependent complaints in the area of the calcaneus and the sole of the foot showed, different causes with similar symptomatology can manifest clinically. In order to differentiate or confirm the diagnosis, imaging diagnostics are then required after taking the patient’s history, clinical examination and possible laboratory diagnostics in order to enable adequate therapy if the differential diagnosis is clarified. The current topic of apophysitis calcanei also fits into this concept.
Also known as Sever’s injury, Sever’s disease, or Sever-Haglund disease, the change in calcaneal apophysis is most commonly found in children and adolescents with an age peak between 8 and 15 years. It affects children who are (over)active in sports and also those who are overweight. The excessive mechanical stress is the cause of the disease [3–5].
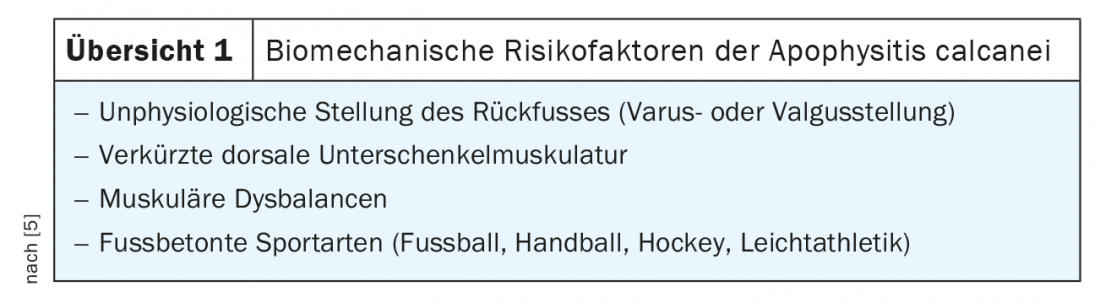
The term apophysitis is misleading and suggests an inflammatory bony change. However, an inflammatory genesis has been refuted. Transient osseous perfusion disturbances, triggered by the mechanical stress, play a causative role. This is due to increased musculotendinous traction by the superficial flexor lodge with consecutive shear forces at the apophysis. Repeated microcontusions of the heel during running or jumping sports can also cause the local stress reaction. Sever’s disease becomes clinically conspicuous especially during growth spurts of the long bones. Various biomechanical risk factors are discussed (review 1), and coprevalence of complaints in the Achilles tendon and plantar fascia have been described.
The painful symptomatology usually occurs in the apophyseal region of the heel in a load-dependent manner, already during or immediately after athletic exertion. The dorsal heel region may be swollen and is tender to pressure. The “one-leg stand” on the affected side, the compression test and the pressure test have a very high sensitivity of pain provocation with a 100% specificity [2].
Therapeutically, conservative measures with reduction of stress, prescription of insoles, and possible support with analgesics have proven effective [2,4].
Radiographs can ideally demonstrate homogeneous or inhomogeneous condensations of the apophysis, occasionally fragmentations. Physiological variants of the apophysis with wavy contour or wide apophyseal cleft must be differentiated. Sonographically, the wide apophyseal gap, inflammatory edematous soft tissue reactions, and Doppler sonographically, local hyperemia can also be detected [5].
Computed tomographic examinations are of more differential diagnostic interest to exclude fractures or osteodestructive processes.
Magnetic resonance imaging clearly shows the local periosteal inflammatory reaction due to the high soft tissue contrast, in particular also the bursitis or tendinitis, as well as the resulting spongiosa edema due to the bony perfusion disturbance. The edema may be very slightly developed, and the hyperintense signal change in fat suppression discrete [1].
Case studies
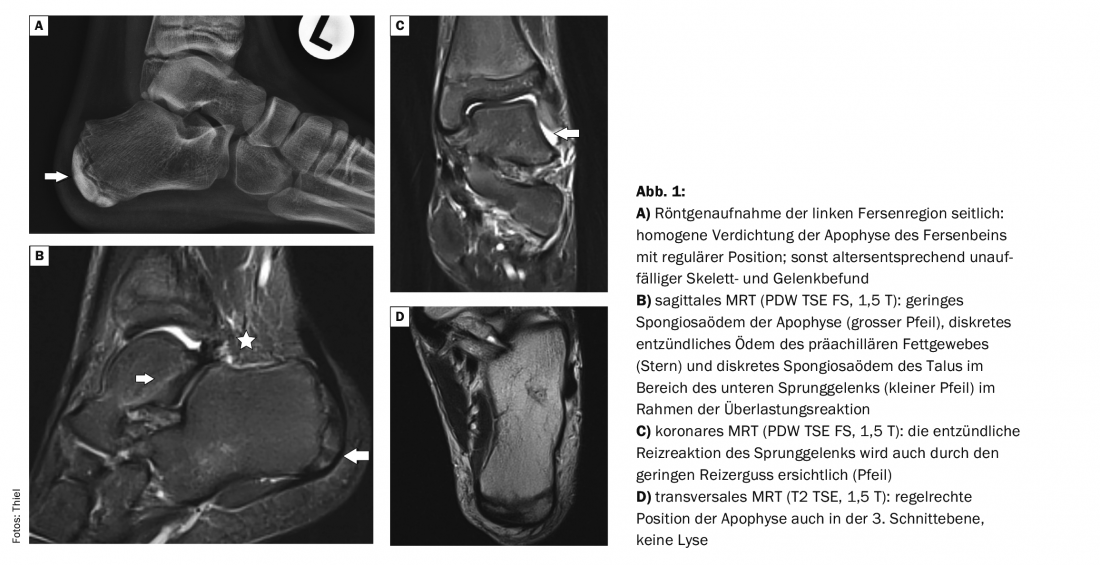
The case example (Fig. 1) shows the imaging studies in a 12-year-old boy, avid soccer player. For the past 3 months, left heel dorsal pain had been occurring immediately after exercise, sometimes even with normal walking. The radiograph was requested to rule out a fracture for “unclear pain condition.” A conspicuous finding was an almost homogeneous compression of the apophysis of the calcaneus with regular position (Fig. 1A). 6 days later, with the suspicion of apophysitis, MRI was performed to verify the findings. This revealed only discrete edema of the cancellous bone of the apophysis (Fig. 1B) and an irritation effusion in the ankle joint (Fig. 1C). The normal position between the apophysis and the corpus calcanei could also be confirmed in the transverse scan (Fig. 1D).
Take-Home Messages
- Apophysitis calcanei is not a true inflammatory disease of the calcaneus, but rather a microtrauma with consecutive perfusion disturbance and cancellous bone edema.
- Apophysitis can be diagnosed anamnestically and by clinical examination; imaging techniques have primarily differential diagnostic value.
- Preferably affected are children and adolescents who are active in sports and also overweight.
- In addition to the mechanical stress on the apophysis caused by the tendon pull of the superficial flexors of the lower leg, the cause is an ankle joint misstatics and musculotendinous imbalance.
- Conservative therapy measures with consistent relief and supportive medicinal analgesic-antiphlogistic objectives are usually sufficient.
Literature:
- Fischer W: MR-Atlas.com, mr-Verlag: Zusmarshausen, 2014 (550).
- Perhamre S, et al: Sever’s injury: treatment with insoles provides effective pain relief. Scand J Med Sci Sports 2011; 21(6): 819-823.
- Perhamre S, et al: Sever’s injury: a clinical diagnosis. J Am Pediatr Med Assoc 2013; 103(5): 361-368.
- Perhamre S, et al: A heel cup improves the function of heel pad in Sever’s injury: effects on heel pad thickness, peak pressure and pain. Scand J Med Sci Sports 2012; 22(4): 516-522.
- Hotfiel T, Forst R: Sever-Haglund disease, www.springermedizin.de/emedpedia/orthopaedie-und-unfallchirurgie (last accessed Oct. 21, 2021).
HAUSARZT PRAXIS 2021; 16(11): 42-44









