Anxiety disorders are among the most common mental illnesses. In addition to psychotherapeutic measures, a wide range of pharmacological agents is available today. These two forms of treatment can also be used in combination. The overall goal is to improve everyday coping and quality of life.
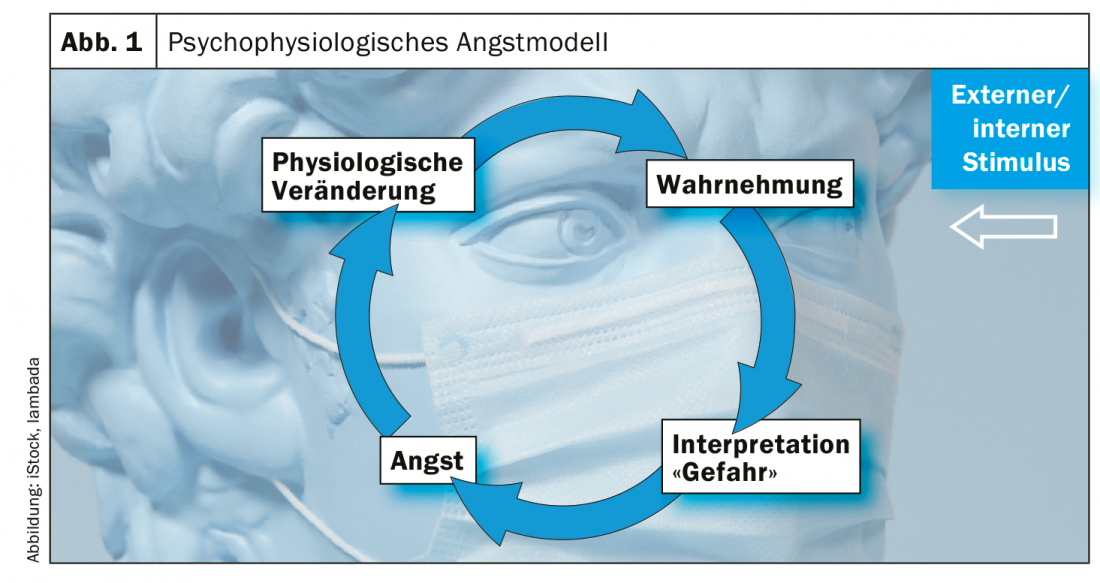
In Switzerland, every second person is affected by a mental illness, either directly or in their circle of relatives/acquaintances, explains Nina Schweinfurth, MD, senior physician at the UPK Basel [1]. The lifetime prevalence of anxiety disorders is up to 20%. Often the primary care physician is the first point of contact, and general medical care plays an important role. A careful anamnesis forms the basis for the diagnosis; it is also important to exclude somatic causes for the complaints. One criterion for distinguishing non-pathological anxiety from dysfunctional anxiety symptomatology is, in addition to subjective suffering, a non-existent connection to an objective threat, including impairment in everyday professional or private life. In addition to the cognitive-affective level (e.g., catastrophizing) and behavioral aspects (e.g., avoidance), physical symptoms (e.g., palpitation, sweating) often occur. It can lead to a vicious cycle of escalating perceptual and physiological components of anxiety, combined with feelings of uncontrollability (Fig. 1).
Pharmacotherapy as an element of a multimodal treatment concept
The overall therapeutic goal is to promote the patient’s functional ability and quality of life. This is to be achieved by providing relief from anxiety symptoms, both at the affective and at the cognitive and autonomic levels. Linked to this is a reduction in avoidance behavior. A multimodal therapy has proven effective for anxiety disorders. Psychoeducation is an important component. In the process, connections are conveyed about vegetative, cognitive and affective levels of anxiety problems. Lifestyle factors, imprints, and the issue of psychosocial resources will be highlighted. It has been shown that the combination of psychotherapeutic and pharmacological measures can be very effective, explains the speaker [1].
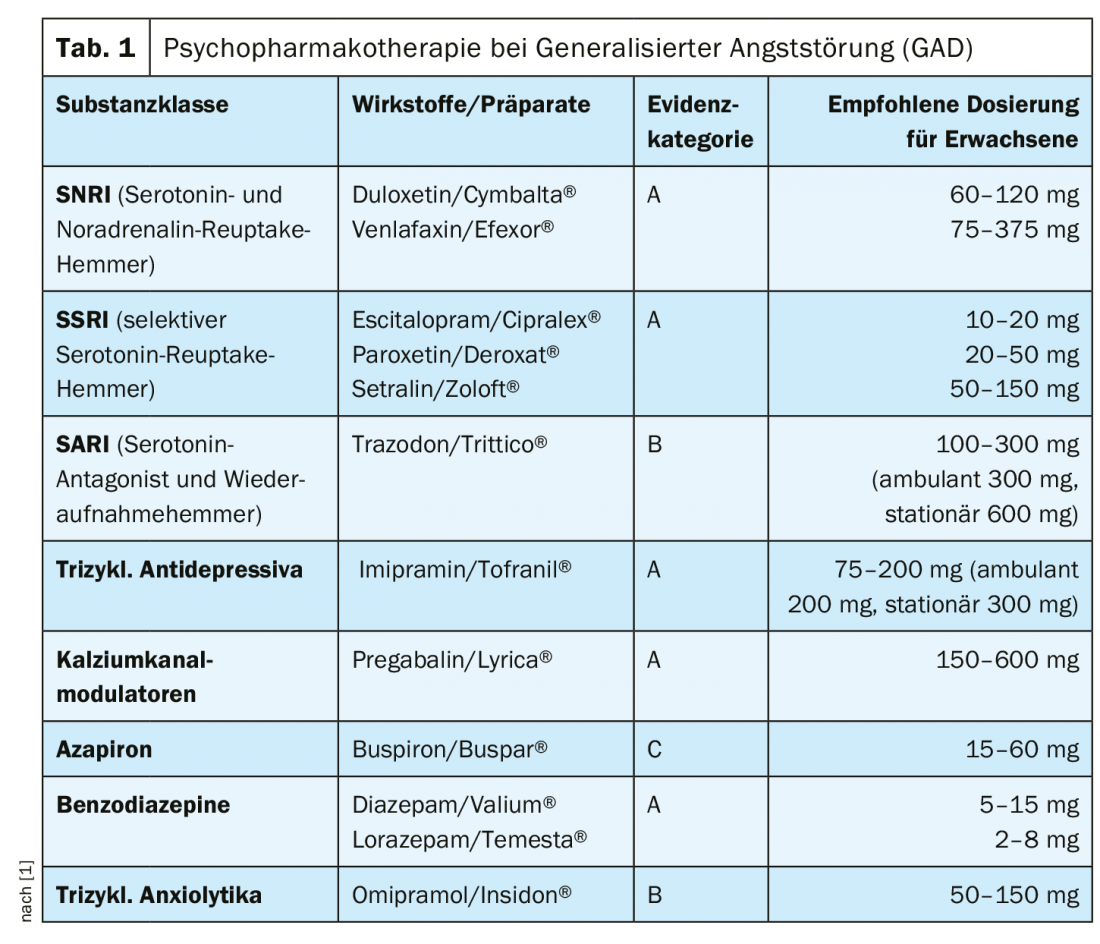
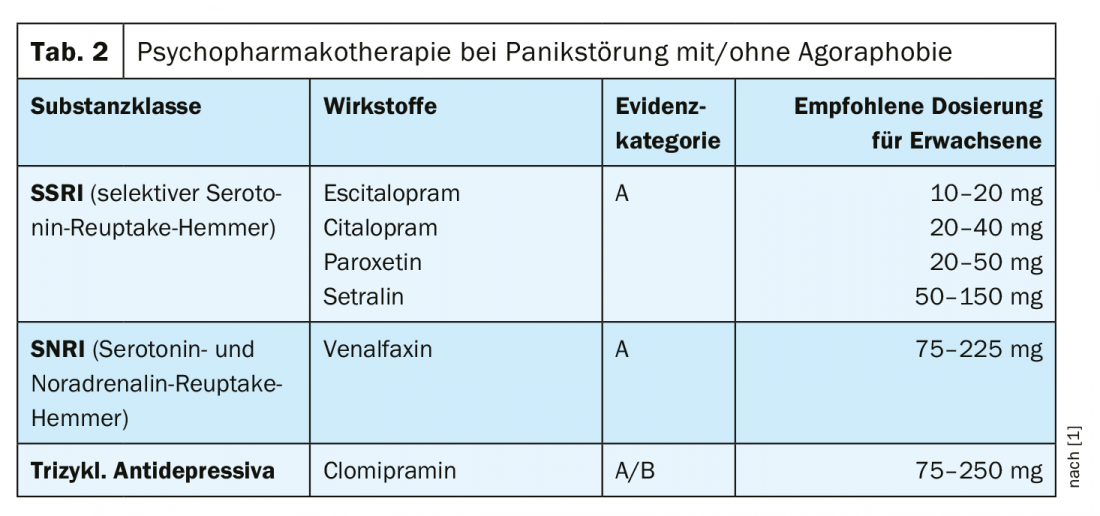
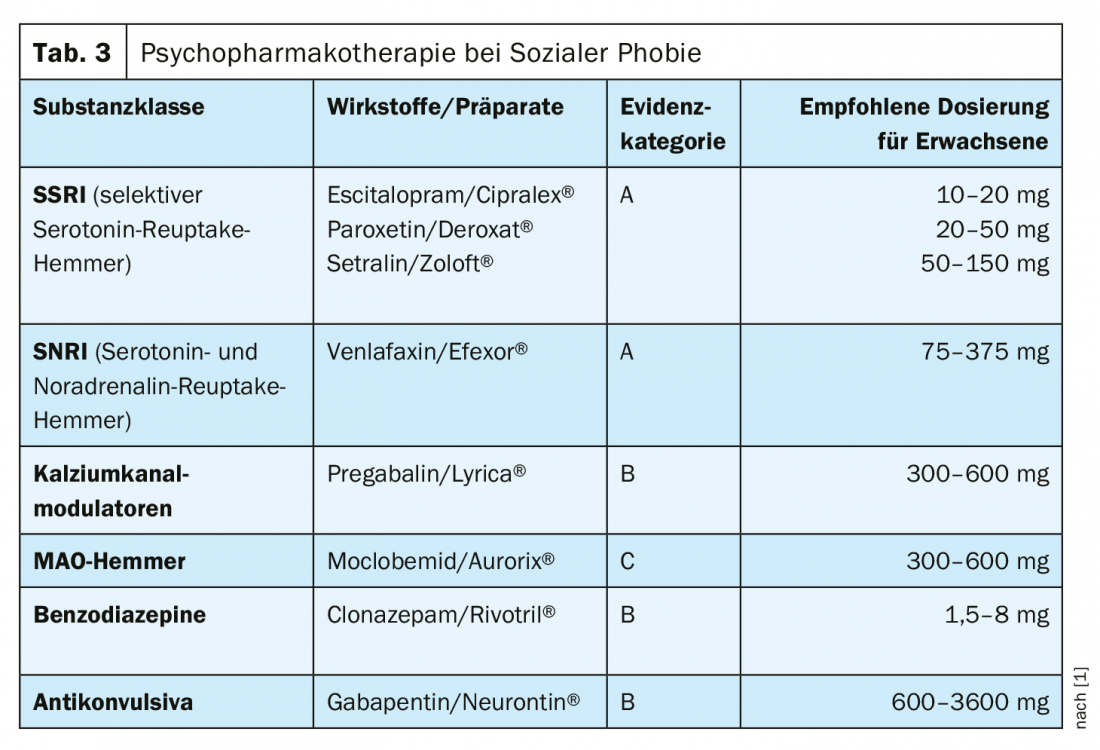
Which psychotherapeutic intervention is appropriate should be determined on an individual basis. According to the expert, there is a large empirical evidence base on the effectiveness of behavioral therapy treatments [1]. An appropriate intervention may include the following elements: Setting goals, conducting a situation analysis, creating an anxiety hierarchy, relaxation procedures and other techniques, and possibly initiating social skills training (especially for social phobic problems). For specific phobias, such as arachnophobia, exposure and relaxation are central behavioral therapy elements; systematic desensitization is sought. With regard to pharmacotherapeutic treatment options, a broad spectrum of substance classes is available today. Dr. Schweinfurth explains specific treatment options for Generalized Anxiety Disorder (GAD) (Tab. 1), Panic Disorder with/without Agoraphobia (Tab. 2 ) and Social Phobia (Tab. 3) . In addition to SSRIs (selective serotonin reuptake inhibitors) and SNRIs (serotonin and norepinephrine reuptake inhibitors), the substance classes SARI (serotonin antagonist and reuptake inhibitor), tricyclic antidepressants, calcium channel modulators, MAO inhibitors, benzodiazepines or tricyclic anxiolytics can be used.
Generalized anxiety disorder (GAD) (ICD 10: F41.1) [2] is characterized by generalized and persistent anxiety symptoms that are not limited to specific environmental stimuli. Common complaints include persistent nervousness, tremors, muscle tension, sweating, lightheadedness, palpitations, dizziness, or upper abdominal discomfort. Often the fear is expressed that the patient himself or a relative might soon fall ill or have an accident. When assessing Generalized Anxiety Disorder (GAD) , Dr. Schweinfurth recommends asking specific questions such as, “Do you often worry about yourself and/or your family?”, “Do you see yourself as someone who generally worries a lot?”, “Does this cause impairment or conflict in your daily life?”. The GAD-7 (Generalized Anxiety Disorder 7) is suitable as a brief structured screening tool; it is a module of the Patient Health Questionnaire (PHQ-D) [3]. The spectrum of pharmacotherapeutic treatment options is shown in Table 1.
Panic disorder with/without agoraphobia (ICD 10: F41.0) [2] is characterized by recurrent panic attacks and a fear of catastrophic consequences. This is associated with a persistent apprehension of suffering such attacks (anticipatory anxiety) and may result in marked avoidance behavior, which may lead to agoraphobia. As with other anxiety disorders, key symptoms include sudden onset of palpitations, chest pain, feelings of suffocation, dizziness, and feelings of alienation. There is comorbidity with other anxiety disorders, depression, and substance dependence (e.g., medications, alcohol). Psychomarmacotherapeutic options are summarized in Table 2 .
Social phobia (ICD 10: F40.1) [2] focuses on a persistent and unreasonable fear of negative evaluation by other people and associated avoidance behavior of social situations. Those affected fear embarrassment and being negatively evaluated. Most often, sufferers have low self-esteem. At the physiological level, flushing, hand tremors, nausea, or urination may occur. Sometimes panic attacks can occur. In its most pronounced form, social phobia leads to isolation. The psychotropic drugs that can be used to relieve symptoms can be seen in Table 3.
Source: FOMF Basel 2020
Literature:
- Schweinfurth N: Anxiety disorders: modern therapies. Nina Schweinfurth, MD, FOMF Basel, Jan. 31, 2020.
- International Statistical Classification of Diseases and Related Health Problems (ICD-10), www.icd-code.de.
- Löwe B, et al: Patient Health Questionnaire (PHQ D). Complete version and short form. Test folder with manual, questionnaires, templates. 2nd edition. Karlsruhe: Pfizer 2002.
- Swiss Archives of Neurology, Psychiatry and Psychotherapy, Role of (epi-)genetic and endocrine markers in the etiology, diagnosis and treatment of depressive and anxiety disorders – current state of research and future developments Dr. Susanne Fischer,
- Prof. Dr. Ulrike Ehlert, Univeristät Zürich, Psy-Congress, 04-06.09.2019. Course 9, https://sanp.ch/fileadmin/content/supplements/SANP_Suppl_8.pdf
HAUSARZT PRAXIS 2020; 15(8): 42-43 (published 8/15/20, ahead of print).