
Misdiagnosed pneumonia in hospitalized adults is not uncommon, especially in older people with geriatric syndromes, but can be very damaging. Little is known about the incidence, risk factors and consequences associated with the misdiagnosis of community-acquired pneumonia.
Lower respiratory tract infections, including community-acquired pneumonia ( CAP), are the fourth leading cause of hospitalization and the most common infection-related cause of hospitalization in the United States. While some incorrect diagnoses of CAP are unavoidable due to diagnostic uncertainty when patients are first admitted, many patients remain misdiagnosed even when discharged from the hospital. Misdiagnosis of CAP can harm patients through delayed recognition and treatment of acute (e.g. heart failure exacerbations), chronic or newly diagnosed conditions (e.g. lung cancer) and lead to unnecessary antibiotic use, side effects and antibiotic resistance. Precisely quantifying the proportion of patients treated for CAP who have been misdiagnosed is a challenge due to the lack of validated definitions. Prof. Dr. Ashwin B. Gupta, University of Michigan Medical Center, Ann Arbor, and his colleagues developed a metric to quantify CAP misdiagnosis that was validated by the National Quality Forum (NQF). They then applied this metric to a prospective cohort study of hospitalized patients treated for CAP at 48 Michigan hospitals to understand the epidemiology and outcomes associated with a CAP misdiagnosis [1]. Hospitalized patients treated for CAP between July 1, 2017 and March 31, 2020 were evaluated. Adults who were discharged with a diagnosis of pneumonia and received antibiotics on the first or second day of hospitalization were included. An unwarranted CAP diagnosis was defined using the National Quality Forum recommended metric as CAP-directed antibiotic therapy in patients with fewer than 2 signs or symptoms of CAP or negative chest imaging. Risk factors for inappropriate diagnosis were assessed, and 30-day composite outcomes were documented for inappropriately diagnosed patients and stratified by full (>3 days) vs. short (≤3 days) antibiotic treatment. The 30-day composite outcomes were defined as mortality, readmission, emergency room visit, Clostridioides difficile infectionand antibiotic-associated adverse events.
Incorrect diagnoses, especially for older people and people with dementia
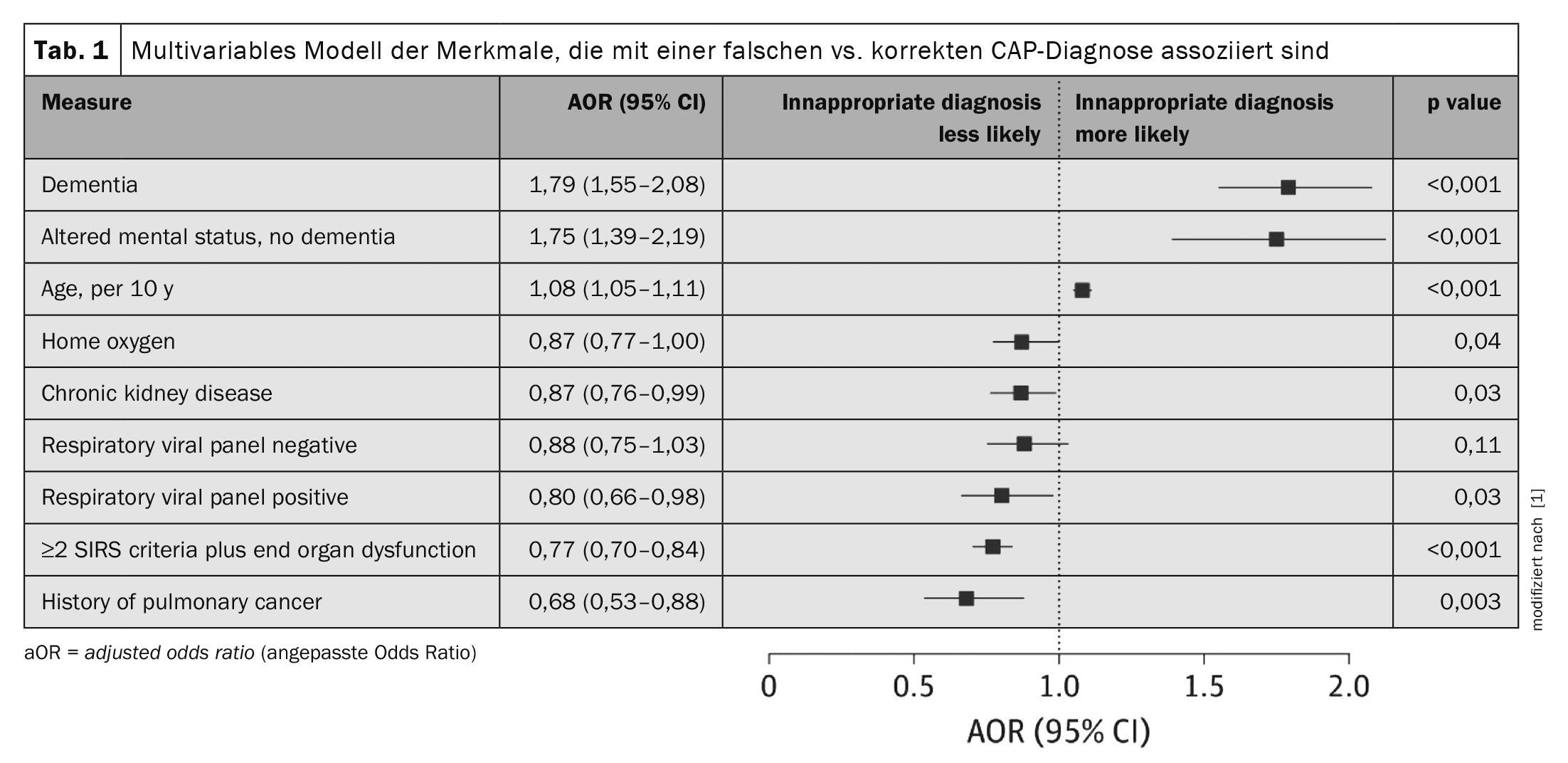
Of the 17 290 hospitalized patients treated for community-acquired pneumonia, 2079 (12.0%) met the NQF criteria for an incorrect diagnosis. The mean (SD) percentage of patients treated for CAP who were incorrectly diagnosed varied by hospital (12.8% [5,4%]), with 30 of 48 hospitals (62.5%) incorrectly diagnosing 10% or more of patients with CAP. Of the 2079 patients who were inappropriately diagnosed with CAP, 1531 (73.6%) had no radiologic criteria, 507 (24.4%) had fewer than 2 signs or symptoms of pneumonia, and 41 (2.0%) met neither criterion. Computed tomography of the chest was performed in 42.1% of all patients. As in patients with CAP, dyspnea and/or cough were most common in the misdiagnosed patients. In the bivariable analysis, patients with misdiagnosed CAP were older (≥75 years) compared to patients with CAP and were more likely to have statutory health insurance, have an altered mental status on admission, have limited mobility (e.g. bedridden, wheelchair dependent) or have been hospitalized within the last 90 days. Regardless of the living situation on admission (e.g. at home or in a care facility), patients diagnosed with CAP were more likely to be admitted to a care facility. In a multivariable analysis, patients with an incorrect diagnosis were older compared to patients with CAP (adjusted odds ratio, aOR, 1.08; 95% CI 1.05-1.11; p<0.001 per decade) and were more likely to have dementia (aOR 1.79; 95% CI 1.55-2.08; p<0.001) or to present with altered mental status without dementia (aOR 1.75; 95% CI 1.39-2.19; p<0.001) (Tab. 1).
Misdiagnosed CAP patients associated with antibiotic-related adverse events
Patients who were incorrectly diagnosed with CAP received a median (IQR) of 7.0 (5.0-9.0) days of antibiotics, of which 4.0 (3.0-5.0) days were as inpatients. The majority of misdiagnosed patients (87.6%, n=1821) received a full course of antibiotics. On bivariable analysis, patients treated with full or short empirical antibiotic therapy were more likely to be white (75.0% vs. 66.7%), have a history of COPD (44.6% vs. 35.3%) or have a concurrent COPD exacerbation (28.2% vs. 15.1%). On multivariable analysis, concurrent COPD exacerbation was associated with full vs. short course antibiotic therapy (aOR 1.74; 95% CI 1.13-2.68; p=0.01), while hemodialysis and negative procalcitonin (vs. those not tested) were associated with short course therapies (aOR 0.29; 95% CI 0.20-0.41; p<0.001 and aOR 0.47; 95% CI 0.32-0.68; p<0.001, respectively) The composite outcome of an adverse event within 30 days of discharge occurred in 536 of 2079 patients (25.8%) who were incorrectly diagnosed with CAP. Complete or brief empirical antibiotic therapy in patients incorrectly diagnosed with CAP was not associated with 30-day composite outcomes in either unadjusted or adjusted analyses (aOR 1.00; 95%CI 0.78-1.29; p=0.99: For individual 30-day outcomes, only physician-documented antibiotic-associated adverse events were associated with complete or brief therapy in unadjusted (31 of 1821 [2,1%] vs. 1 of 258 [0,4%]) and adjusted (aOR 7.23; 95% CI 1.18-44.35; p=0.03) analyses.These results showed that an incorrect diagnosis of pneumonia was made in about one in eight patients and in most hospitals the incorrect diagnosis of pneumonia was made in more than 10% of patients. Overall, nearly 88% of patients incorrectly diagnosed with community-acquired pneumonia received a full course of antibiotics associated with physician-documented antibiotic-associated adverse events.
Doctors tend to make “cognitive errors”
According to Prof. Gupta and colleagues, one reason for the misdiagnosis of CAP is that CAP is common and physicians are at high risk for cognitive errors such as “accessibility bias” (i.e. the tendency to make decisions based on the information that comes most easily to mind). Secondly, the symptoms of CAP are non-specific and may overlap with other cardiopulmonary conditions (e.g. exacerbation of heart failure), making diagnosis difficult. In addition, given the poor outcomes associated with CAP in an environment of uncertainty, healthcare professionals may prefer to overtreat a potentially overlooked CAP diagnosis. Third, historical quality indicators imposed by organizations such as the Joint Commission in the US (e.g., the requirement to administer antibiotics within 6 hours) may have inadvertently led to more CAP misdiagnoses. These measures may continue to influence the diagnostic behavior of healthcare professionals. Finally, previously published data show a correlation between CAP misdiagnosis and UTI misdiagnosis at the hospital level, suggesting that local policies, procedures or culture may influence accurate diagnosis. Unsurprisingly, older patients, particularly those with cognitive impairment, were more likely to be misdiagnosed. Patients with cognitive impairment may have difficulty communicating. Therefore, physicians may rely on non-specific data (e.g. white blood cell count, fever) to make a CAP diagnosis. Older adults, particularly those with dementia or altered mental status, are also more likely to be misdiagnosed with other conditions, such as a urinary tract infection (i.e. asymptomatic bacteriuria). While altered mental status can be a sign of infection, even severe infection, it has a wide range of differential diagnoses (e.g., polypharmacy, pain, dehydration), and focusing on CAP can delay correct diagnosis and treatment. Finally, because older patients with CAP tend to have poorer health outcomes, there is an increased tendency to quickly diagnose and treat suspected CAP, leading to higher rates of misdiagnosis, the authors conclude. In patients at high risk for poor outcomes due to delayed treatment of CAP, it may be reasonable to prescribe antibiotics empirically while diagnostic evaluation is completed, the experts write. In these populations, guidelines recommend review, de-escalation and discontinuation of antibiotics within 48 to 72 hours once infection has been ruled out. However, the present study found little evidence for stopping antibiotics. Rather, patients who received empirical antibiotic therapy for suspected CAP usually received a full course of antibiotics. Compared to short courses of empirical antibiotics, full courses of antibiotics were found to be associated with antibiotic-associated adverse events. Nevertheless, it is known that prolonged use of antibiotics is associated with increased morbidity and delayed diagnosis of underlying diseases, Prof. Gupta et al. emphasized. Older patients in particular, who may suffer from several diseases at the same time or are more likely to take drugs that interact with antibiotics, are at high risk of harm from antibiotics and delayed diagnosis.
Literature:
- Gupta AB, Flanders SA, Petty LA, et al: Inappropriate Diagnosis of Pneumonia Among Hospitalized Adults. JAMA Intern Med 2024; 184(5): 548-556; doi: 10.1001/jamainternmed.2024.0077.
InFo PNEUMOLOGY & ALLERGOLOGY 2024; 6(4): 34-35









