Gambling is an ancestral leisure activity consisting in irreversible bet of money in a hazard-driven setting. Gambling disorder (GD) is characterized by persistent and recurrent maladaptive gambling behaviour. It shares similarities with substance use disorders. All should be taken into account to design better treatment strategies. Treatment accessibility and early detection are the current challenges.
Gambling is an ancestral leisure activity consisting in irreversible bet of money in a hazard-driven setting. Gambling disorder (GD) is characterized by persistent and recurrent maladaptive gambling behaviour recently acknowledged in the DSM-5 [1] as a behavioural addiction and included in beta draft of ICD-11 [2] among disorders due to addictive behaviors. This decision was supported by scientific evidence on its closeness to substance use disorders (i.e. clinical picture, brain origins, co-morbid-conditions and treatment options).
Epidemiological data
In Switzerland, life-time prevalence of GD in general population aged over 18, ranges from 1,1% for pathological gambling to 2,2% for problem gambling (less number of fulfilled criteria), and 5,5% of Swiss adolescents have been found to be at-risk for GD [3].
Problem gambling shares the natural course with substance use disorders (SUDs), with a chronic course made of relapse and remission periods [4]. It is highly co-occurring with other mental disorders, such as nicotine dependence (60,1%), SUDs (57,5%), mood disorders (37,9%), anxiety disorders (37,4%) and increased suicidal risk [5]. These could be preexistent to GD or appear during its course in longitudinal designs (as found in anxiety and mood disorders) [4].
GD is a source of suffering for the subject and his relatives, resulting in direct health costs (including suicide, and increased health risk resulting from comorbidities with other mental illnesses), but also in indirect costs related to functional impairment (e.g. professional, social and financial impact). In Switzerland the overall social cost of GD has been estimated to be between 551 and 648 million Swiss francs [3].
Neurobiological correlates
The main neural systems hypothesized to be involved in addictive behaviors are the dopaminergic system for reward seeking and the serotoninergic system for emotional regulation. GD seems to share these neurobiological correlates [6]. For dopaminergic involvement for example, the arising question is whether behavioral addictions such as GD, are sufficient rewarding conditions to lead to addiction at the same extent as SUDs, if they lack the potent rewarding exogenous drug intake [7]. The origin of response seems to reside in rather qualitative than quantitative rewarding power (i.e. the potency of reinforcing factors associated to gambling behavior), in addition to learning biases (e.g. preeminence of positive rewards anticipation even after experienced repetitive losses), and inner vulnerability factors (such as impulsivity traits and sensation seeking) [7]. Moreover, data supporting serotoninergic dysfunction in GD, consists in reduced levels of serotonin metabolite in cerebrospinal fluid and in reduced serotonin activity, which are linked to GD severity [4].
Psychological mechanisms
Neurobiological dysfunctions in GD are reflected by clinical symptoms such as patterns of control loss towards time and money spending. Dysfunctional motivational processes are key factors. Gambling is a source of powerful sought sensations (e.g. arousal before gambling, expected monetary rewards, dissociation and immersion during gambling). But it could also become a maladaptive coping behavior to aversive affects or thoughts, with mood related facets of impulsivity (i.e. urgency) and deficits in response inhibition, similarly to cocaine-dependent subjects [7].
Moreover, motivational context is added to specific cognitive distortions under probabilistic conditions, leading to gambling continuation despite repeated losses. GD’s cognitive biases mainly consist in illusion of control (i.e. overestimation of one’s own influence over random outcomes) and in recurrent attempts, through gambling, to recover from previous financial losses (i.e. chasing) [7]. Disordered gamblers are prone to risky decision-making and insensitivity to feedback of impulsive choices made [7]. Moreover, gambling high-craving cues reverse the usual subjective value-coding pattern and conduce to more impulsive choices [7]. The propensity for cognitive distortions in disordered gamblers is reinforced through gambling offer characteristics, and increases loss of control. Near misses for example (often used in gambling offer), activate brain regions related to wins in spite of those related to losses [7]. This cognitive distortion can partly explain the learning process failure (i.e. absence of extinction of gambling behavior despite repetitive loss experiences) within disordered gamblers.
The potent incentive nature of gambling added to its physiologically arousing intensity can lead a minority of gamblers to lose control and engage in a problematic repeated behavior. They are driven by unsuccessful attempts to apply learning rules (i.e. the more you train, the more you become skilled) to a random activity. Seeking the «chance» to make an «easy big win» could represent the addictive ingredient in GD (stackable to neurobiological drug effects) [7].
Assessment tools and challenges
Gambling disorder and its related social and financial harms should be assessed, diagnosed and treated. Only a minor proportion (less than 3%) of subjects suffering from GD, is in treatment [8]. The major reported motivators to seek treatment were important financial and interpersonal harms resulting from GD, and barriers to seek help were mainly inner to the patient (e.g., shame and conviction in own capacity to handle) [8]. Primary health professionals are a cornerstone of early detection of GD and its financial and psychological harms (including suicidal risk) and of patients’ referral to specialists [8].
«Lie-bet», is a two questions screening tool useful for non-specialized professionals (Fig. 1), easy-to-use in medical practice settings. One positive response implies further specialized assessment. Other screening instruments exist such as South Oaks Gambling Screen (SOGS), a 20 items questionnaire that identifies at-risk gamblers, and The Canadian Problem Gambling Index (CPGI) which assesses problem gambling severity. The emergence of online gambling offer with a different type and more prevalent related GD, has set questions about adapted identification instruments. Previously described screening tools could be used for online GD, but those tools designed for problematic internet use such as the Internet Addiction Test (IAT) are also suitable [9].
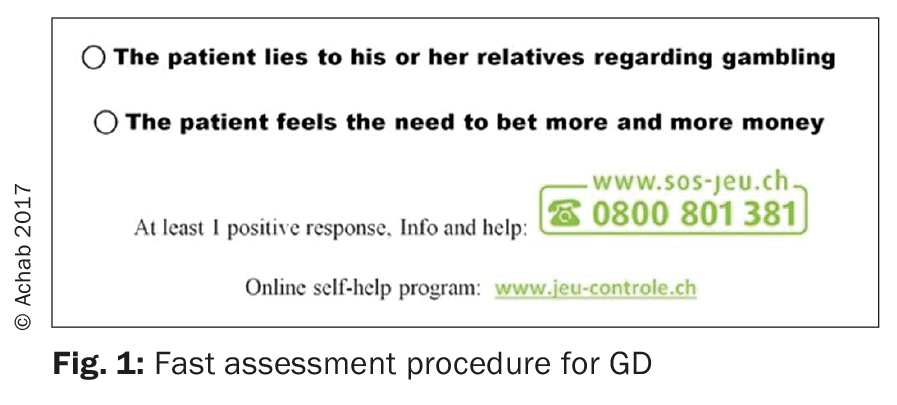
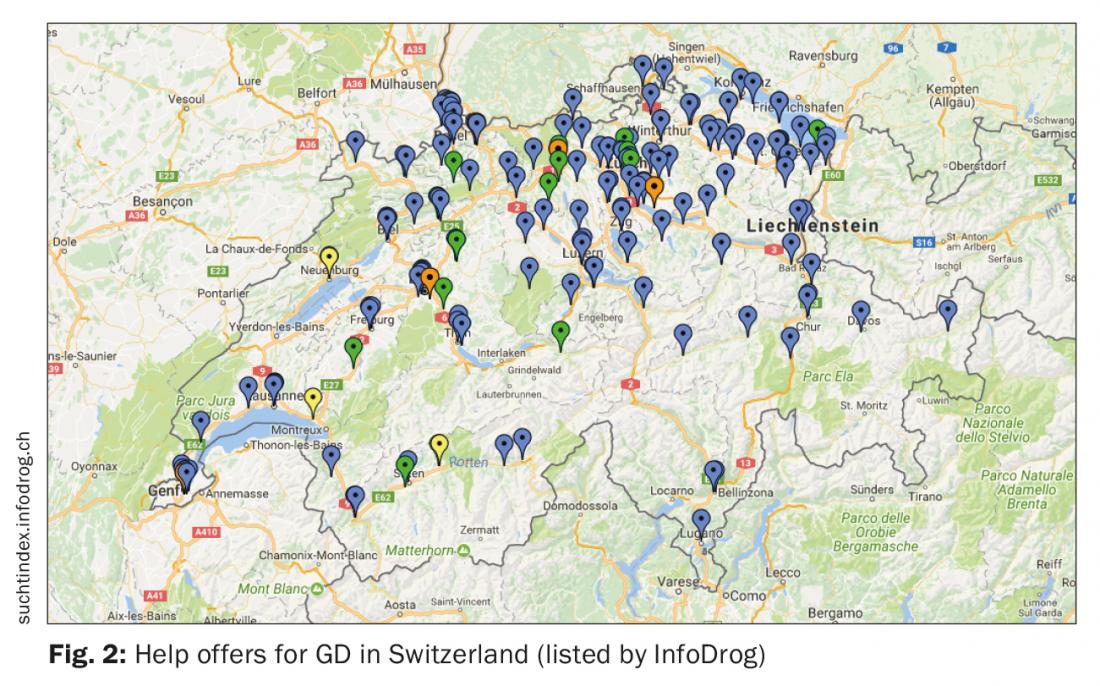
When screened, a patient could be referred to a specialist, as long as the local network of specialized facilities is identified by care professionals. A recent study on Swiss general practitioners knowledge on GD and referral paths, showed that only 7% of the participants screen for GD, and that 32% of this minority lacked knowledge on what to do or where to refer screened patients [8]. To address this issue, we provide in the present article, a fast screening procedure for Swiss professionals (Fig. 1) that we developed. We also provide here for referral purposes or for information needs, a link (https://suchtindex.infodrog.ch/de) to the National website listing facilities in charge of counseling, prevention or treatment of addictive disorders – including GD – ranged by canton and type of offer (Fig. 2).
Specialized psychiatrists can make diagnosis during a structured interview. It could rely on Gambling Disorder criteria from DSM-5 [1] that provides a severity index, or on WHO description for Gambling Disorder [2] that differentiates GD from hazardous gambling and includes predominantly online and predominantly offline forms.
Treatment options
Understanding psychological features of GD, diagnosing and exploring avenues, that could enhance help seeking, are the basis of treatment response that could be offered to subjects with such disorder and to their relatives. In Switzerland specialized facilities have developed over the last decade offering help, counseling and treatment for people affected directly and indirectly by this complex mental disorder [3].
Psychotherapy is the main treatment for GD. It has benefited from psychotherapeutic approaches, mainly those used for SUDs (motivational psychotherapy, brief interventions, cognitive behavioral therapy (CBT), family therapy and support to patient’s relatives) that showed positive results on remission and relapse prevention [7]. Besides these non-specific treatments, specific approaches for GD (i.e., cognitive therapy for gambler’s fallacy and financial problem management) have been developed and are now considered to be efficient treatment options [10]. Psychotherapy is mainly in an individual basis, with some adjusted family and couple interviews. The patient along with his therapist decides a treatment goal according to his own values and objectives in his life project. Treatment focuses on gambling behavior, but more importantly on the psychosocial conditions that favored its development and maintenance (e.g. negative mood coping, sensation seeking, impulsivity, feeling of loneliness, or challenging working place). Co-morbid-conditions are addressed and relapse prevention planed when the predetermined treatment goal has been achieved and consolidated. Rather than focusing on abstinence from gambling, it seems that a more controlled gambling behaviour is a viable and attractive treatment objective for numerous gamblers. Particularly, it was found that gamblers seeking abstinence tend to change their own goal into seeking control, in a one-year follow-up [11].
A pharmacological treatment response is well demonstrated in SUDs for many indications (e.g., detoxification, relapse prevention, and harm reduction), but there is not yet approved pharmacological treatments for pathological gambling. A possible efficacy of opiate antagonist in GD has been replicated in a number of controlled studies [10]. Preliminary results on N-acetyl cysteine, Memantine and Topiramate produced clinical improvement and may open new avenues for treatment [10]. In the absence of co- morbid psychiatric disorder, studies failed to conclude to efficacy of antidepressants, mood stabilizers and antipsychotic drugs on GD [10].
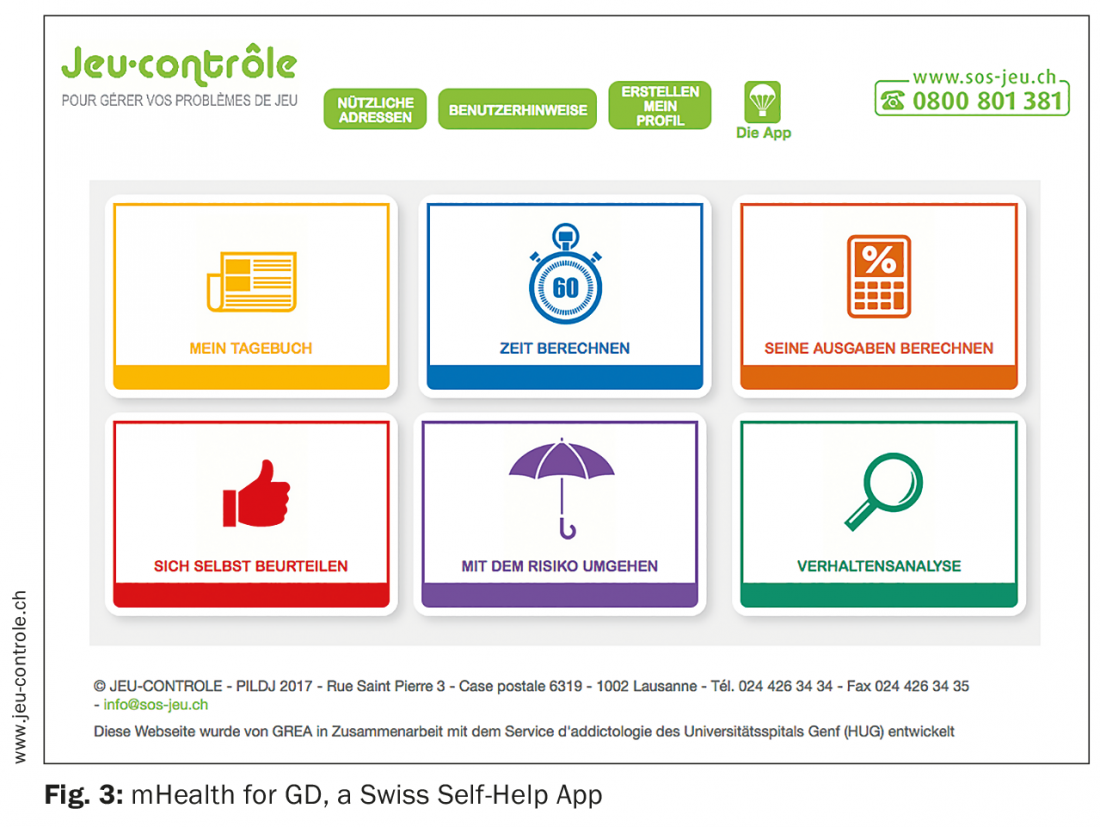
In spite of available treatments, only a very small part of people with GD asks for help. Internet delivered treatments for GD has been shown to be promising [11]. A Swiss mobile App (www.jeu-controle.ch) has recently been launched (Fig. 3). It was developed to help subjects to increase their control over gambling behavior (e.g. time and money spent) and to sustain their motivation to achieve their own goals. They are given a specific personalized feedback reinforcing goal achievements and a visualization of their gambling behavior and mood evolution [11]. The app and the related website could also be used as a complementary resource to face-to-face psychotherapy.
Public health considerations are of importance regarding GD in Switzerland. Prevention and treatment response should be straightened, a recent review paper draws some perspectives [3]. Particular attention should be paid to regulation of risky online gambling offer and to youth protection [7].
Conclusion
Gambling disorder shares similarities with SUDs, but also has its features. All should be taken into account to design better treatment strategies to help patients and their relatives on a personalized basis. Treatment accessibility and early detection are the current challenges. Efforts should be sustained to cope with emerging challenges such as online gambling offer and gamification of gambling that both could put additional population categories at-risk (e.g. youth, women and elderly).
Take-Home-Messages
- A non-problematic gambler: gambles for pleasure, according to his/her financial status, accepts to lose money bet, and never gambles to chase losses.
- Specific features to Gambling Disorder (GD) are gambler’s fallacy and other cognitive biases applied to random conditions related to money incentives, such as chasing, illusion of control and near miss effect.
- Problem gamblers rarely seek treatment despite of negative consequences and suffering, assessment in primary care settings is accordingly of major importance.
- Treatment of GD consists principally in psychotherapy targeting gambler’s fallacies and in debt management.
Bibliography:
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. 5th edition. Washington, DC 2013.
- WHO: Betadraft of ICD-11. [http://apps.who.int/classifications/icd11/browse/l-m/en] 2017
- Billieux J, et al.: Gambling and problem gambling in Switzerland. Addiction 2016; 111(9): 1677–1683.
- Yau YH, Potenza MN: Gambling disorder and other behavioral addictions: recognition and treatment. Harv Rev Psychiatry 2015; 23(2): 134–146.
- Lorains FK, Cowlishaw S, Thomas SA: Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction 2011; 106(3): 490–498.
- Achab S, Karila L, Khazaal Y: Pathological gambling: update on decision making and neuro-functional studies in clinical samples. Curr Pharm Des 2014; 20(25): 4000–4011.
- Achab S: Features of Gambling Disorder and Internet Gaming Disorder in the spectrum of addictive disorders. Thesis; University of Geneva, Psychiatry 2016.
- Achab S, et al.: Early detection of pathological gambling: betting on GPs’ beliefs and attitudes. Biomed Res Int 2014; 2014: 360585. 9.
- Khazaal Y, et al.: Factor Structure of the Internet Addiction Test in Online Gamers and Poker Players. JMIR Ment Health 2015; 2(2): e12.
- Achab S, Khazaal Y: Psychopharmacological treatment in pathological gambling: a critical review. Curr Pharm Des 2011; 17(14): 1389–1395.
- Khazaal Y, et al.: mHealth app for gambling disorder: Rational and description. «Jeu-contrôle», rationnel d’une application de soutien aux limites de jeux. Journal de Thérapie Comportementale et Cognitive 2017; 27(3): 129–137.
Info NEUROLOGIE & PSYCHIATRIE 2017; 15(6): 13–17