Patient satisfaction is an essential pillar for therapeutic success, especially in aesthetic patients. It depends not only on the quality of treatment, but also on the quality of care provided by the doctor and practice staff. This requires good communication between the doctor and the patient and an aesthetic sensibility on the part of the doctor. Patient satisfaction has crucial to do with a good practice structure.
In recent years, it has been recognized that patient satisfaction is a decisive factor for the success of treatment – especially for esthetic patients. But how can high patient satisfaction be achieved with botulinum toxin (BTX) A treatment? This was the subject of a recently published paper by the Swiss Group of Esthetic Dermatology and Skincare (SGEDS), led by Oliver Ph. Kreyden, MD.
In order to achieve the greatest possible patient satisfaction, it is important to keep in mind the special nature of the aesthetic patient: As a healthy self-payer, their expectations are generally higher than those of sick patients seeking help in medical dermatology. Many aesthetic patients desire the treatment of a disturbing blemish with a specific method (demand principle), while the sick patient depends on the doctor’s recommendation and gladly accepts it with hope of cure (help principle). The prerequisite for a fully comprehensive treatment success is that the esthetically active physician, due to his specific training and further education, brings the esthetic patient from the demand principle to the assistance principle through competent and high-quality consultation and that the balance of power between the physician and the esthetic patient is balanced.
Patient classification is useful
Since the outcome of any medical treatment and especially of an aesthetic procedure depends on the primary conditions, a rough classification of aesthetic patients seems useful [1]:
- Age of the patient (25-40 years, 40-60 years, >60 years)
- Preventive vs. corrective treatment
- Psychological characteristics of the patient to the psychiatric patient.
- Technically demanding patients.
It is important to identify patients with excessive expectations in advance. Patients with a psychiatric condition, i.e. Body Dysmorphic Disorder, should not undergo aesthetic treatment. Furthermore, men are more difficult to treat than women.
Demands on doctor, staff and practice
For a satisfactory aesthetic treatment, the attending physician must have the following skills even more than in classical dermatology:
- Professional competence (education and training in classical as well as aesthetic dermatology)
- Social competence (communication skills and empathy)
- Leadership skills (leadership and organizational management).
Even in aesthetic dermatology (the same as in classical dermatology), no treatment may take place without prior expert medical assessment and determination of an exact diagnosis.
As the first and usually the last contact for the patient, the staff is the business card of the practice. The professional staff must be able to benefit regularly from the doctor, but also from external training (communication, telephone training, management, therapy courses).
Hygiene, cleanliness and a professional appearance of the practice are a matter of course.
Crucial: the initial consultation before treatment
Good education during the initial consultation is critical to high patient satisfaction. That is why every physician should insist on performing an initial consultation before the procedure.
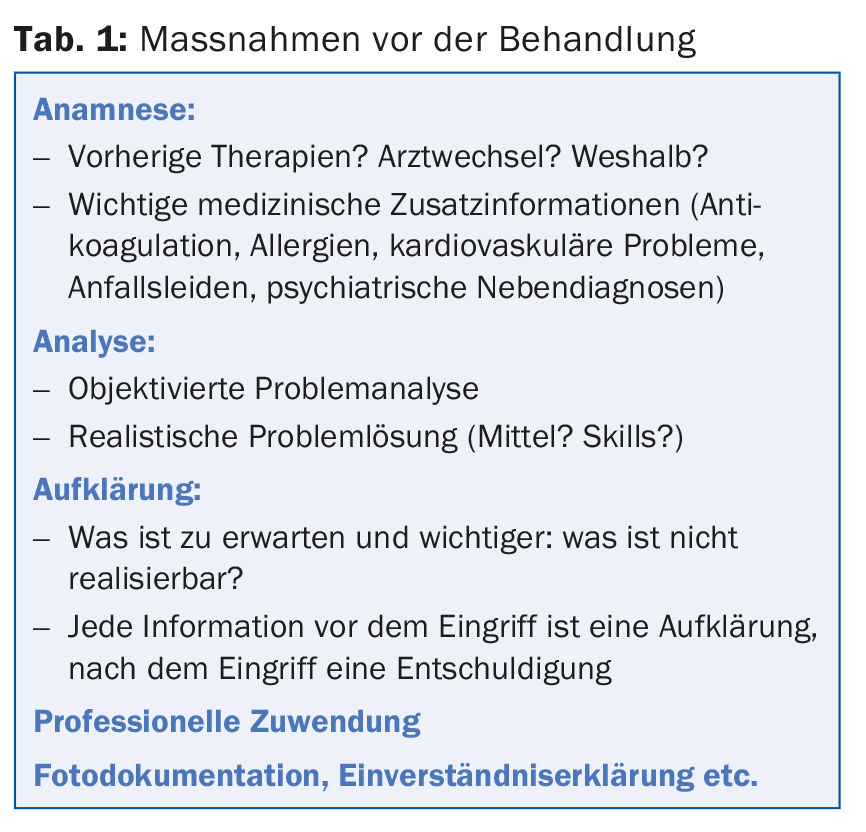
The initial medical consultation serves as a mutual exchange of information and is extremely important for determining the treatment plan, fully informing the patient including possible side effects and financial aspects as well as for the exact timing of the procedure. In addition, this conversation serves to build a basis of trust. As in classical dermatology, it should be divided into history, examination, diagnosis.
A written documented consent and a standardized photo documentation must be created. Table 1 shows an overview of essential factors prior to treatment.
Professional procedure of the actual treatment
In this phase of patient care, the physician’s professional technical skills are primarily in demand, which can be taken from corresponding publications [2–8].
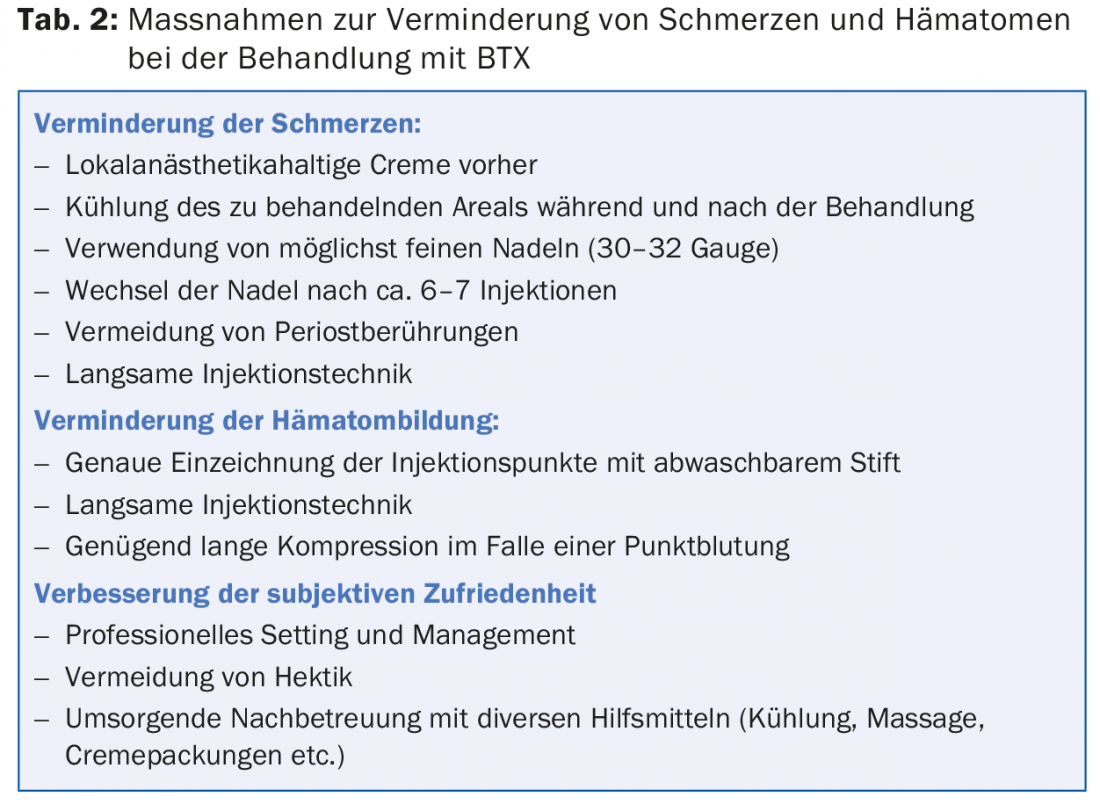
The treating physician should have experience with all three BTX-A preparations approved on the European market. The treatment itself should be made as comfortable and painless as possible for the patient (Tab. 2).
Immediately after treatment, the patient should be given verbal and written information about post-interventional behavior. In case of an initial treatment, it is recommended to make an appointment for a check-up, during which the result will be discussed together and, if necessary, small corrections can be made.
The dissatisfied patient: a challenge for the entire practice team
Even if all the conditions for successful treatment have been met, there are always dissatisfied patients.
The dissatisfied patient must be perceived and, above all, taken seriously by both the staff and the doctor. The staff should be trained in such a way that, in the event of patient dissatisfaction, it is mandatory for them to immediately mediate contact with the attending physician. If patient dissatisfaction is substantiated, the physician must promptly review whether an improvement in outcome is possible and implement it in a timely manner. If improvement can only be achieved by additional measures such as BTX-A injections in additional regions, augmentation, laser or peeling, a new educational consultation is required.
In rarer cases, there is subjective dissatisfaction (the physician is satisfied, the patient is dissatisfied). In the vast majority of cases, this is due to insufficient information provided by the physician during the consultation. Before-and-after pictures as well as fully understanding and competent care with pointing out possible solutions (e.g. micro post-injections) help to convince the patient of the correctness of the treatment.
Constructive handling of complications
As a general rule, what can be corrected should be corrected! The case is more difficult when overcorrection or an uncorrectable complication such as eyelid or eyebrow ptosis occurs.
Positive emotional attention with clear communication of competence often causes a relaxation of the situation. In any case, it is advisable to deal with inconveniences in the office and to take care of patients and their (understandable) concerns. In all cases, dismissal and trivialization are the worst solutions to problems.
Overall, therapy with BTX-A is a treatment that is per se accompanied by high patient satisfaction [9,10]. The measures recommended here succeed in minimizing the already small proportion of dissatisfied patients after treatment with BTX-A.
Source: Kreyden OP, et al: The satisfied patient in aesthetic dermatology. Der Hautarzt 2015; 66(2): 131-136.
Literature:
- Kreyden OP: The patient as a challenge. On dealing with difficult patients in aesthetics. In: Ruzicka T, et al. (Eds.): Progress in Practical Dermatology and Venereology. Springer 2010: 323-329.
- Carruthers J and the Botox Consensus Group: Aesthetic Considerations. In: Consensus Recommendations on the use of botulinum toxin type A in facial aesthetics. Plas Reconstr Surg 2004; 114(Suppl 6): 1S-22S.
- Imhof M, Podda M, Sommer B: Aesthetic botulinum toxin therapy. Guideline of the German Dermatological Society (DDG), German Society for Dermatosurgery (DGDC), German Society for Aesthetic Botulinum Toxin Therapy (DGBT). AWMF 2013; Register No.: 013-077. www.awmf.org/leitlinien/detail/ll/013-077.html.
- Kane M, et al: Expanding the use of neurotoxins in facial aesthetics: A 2 panel’s assessment and recommendations. J Drugs Dermatol 2010; 9(Suppl 1): 1-25.
- Philipp-Dormston WG, Bergfeld D, Sommer B, and the Onabotulinumtoxin Consensus Group: consensus recommendations for treatment with onabotulinumtoxin A in aesthetic medicine. JDDG 2013; 11(Suppl 1): 1-42.
- Raspaldo H, et al: Upper- and mid-face anti-aging treatment and prevention using onabotulinumtoxin A: the 2010 multidisciplinary French consensus – part 1. J Cosmet Dermatol 2011; 10: 36-50.
- Raspaldo H, et al: Lower-face and neck antiaging treatment and prevention using onabotulinumtoxin A: the 2010 multidisciplinary French consensus – part 2. J Cosmet Dermatol 2011; 10: 131-149.
- Rzany B, et al: Recommendations for the best possible use of botulinum neurotoxin type a (speywood units) for aesthetic applications. J Drugs Dermatol 2013; 12: 80-84.
- Fagien S, Carruthers JD: A comprehensive review of patient-reported satisfaction with botulinum toxin type a for aesthetic procedures. Plast Reconstr Surg 2008; 122: 1915-1925.
- Rzany B, Ascher B, Monheit G: Treatment of glabellar lines with botulinum toxin type A (Speywood Unit): a clinical overview. J Eur Acad Dermatol Venereol 2010 Jan; 24(Suppl 1): 1-14.
DERMATOLOGIE PRAXIS 2015; 25(2): 28-31









