Rheumatoid arthritis (RA) is associated with a high level of suffering for those affected and, if left untreated, can lead to disability. Below, Ioannis Papadopoulos, MD, presents a case in which a 54-year-old food service worker with several years of severe RA achieved the therapeutic goal of ongoing freedom from symptoms with the help of a Janus kinase (JAK) inhibitor.

Patient profile
- Male, born 1965
- Service staff in the catering industry
- No other chronic diseases in the medical history
- Family history: mother with RA
- Since 2017: polyarthralgia of the hands
History: First signs of RA since 2017 and presentation to primary care physician.
- In July 2017, the patient complained of increasing functional limitations and pain in fingers II to V of the left hand for 3 months. Due to his many years as a drummer, his ailments have been associated with microtrauma for decades.
- An MRI scan of the left hand showed moderate arthrosis in the distal interphalangeal (DIP) joints II to V, most clearly in the DIP joint V. In addition, moderate osteoarthritis was evident in the proximal interphalangeal (PIP) joint V. The degeneration also revealed mild capsular swelling or signal elevation of the collateral ligaments of the PIP, DIP, and partially metacarpophalangeal (MCP) joints, as well as isolated small intraosseous ganglia. These clarifications were taken over and performed by the patient’s primary care physician.
09/2019: Onset of severe polyarthralgia in both hands.
- In September 2019, the patient developed severe polyarthralgias in both hands.
11/2019: Diagnosis of seropositive RA
- In November 2019, the patient was referred to us for the first time for rheumatologic evaluation and treatment for his symptoms. Marked acute polyarthritis in MCP joints II to III bilaterally, PIP joint III left, right shoulder, and right knee was clinically noted.
- The radiograph of the hands (Figure 1) showed erosion at the radial edge of the head of the middle phalanx of digitus III and joint swelling at the PIP of digitus III on the left. On the right, there were minor erosive changes at the lateral head of the 2. and 3rd ray at the MCP joints as well as general periarticular osseous demineralization.
- Disease activity was classified as high based on a DAS28-CRP value of 5.7. This score was composed of 7 painful joints (Figure 2), 6 swollen joints, a C-reactive protein (CRP) level of 37.4 ml/l, and a patient global health score of 90.
- Laboratory testing revealed an elevated anti-cyclic citrullinated peptide (CCP) antibody and a positive rheumatoid factor in addition to an elevated CRP level (Table 1).
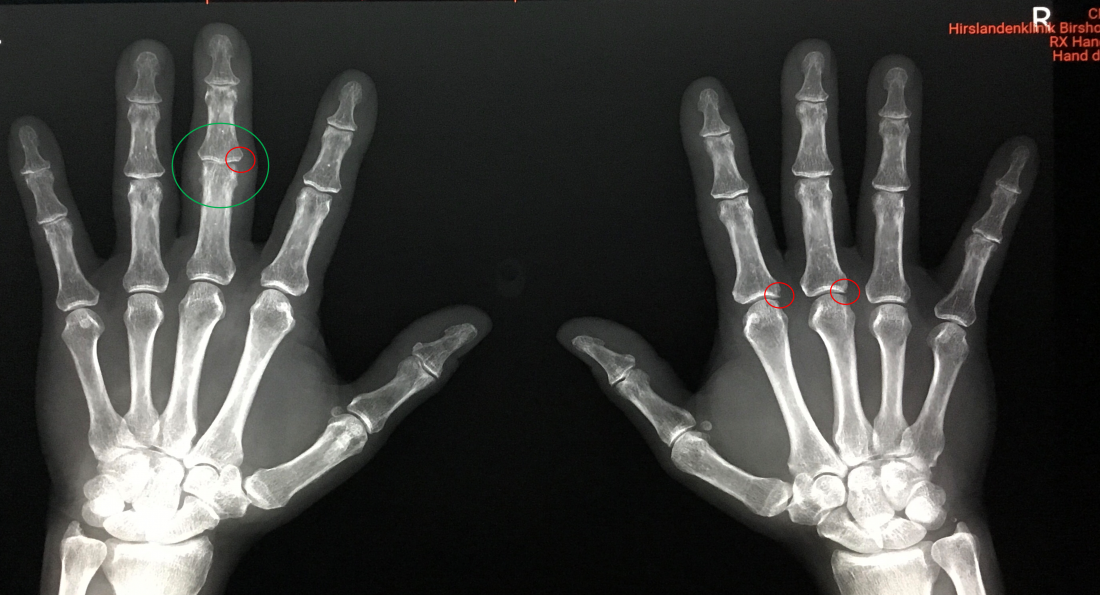 Figure 1: X-ray of both hands 11/2019
Figure 1: X-ray of both hands 11/2019
Left: Erosion at the radial margin of the head of the middle phalanx of digitus III. Joint swelling at the PIP of digitus III.
Right: The MCP joints show minor erosive changes at the lateral head of the 2. and 3rd ray as well as general periarticular osseous demineralization.
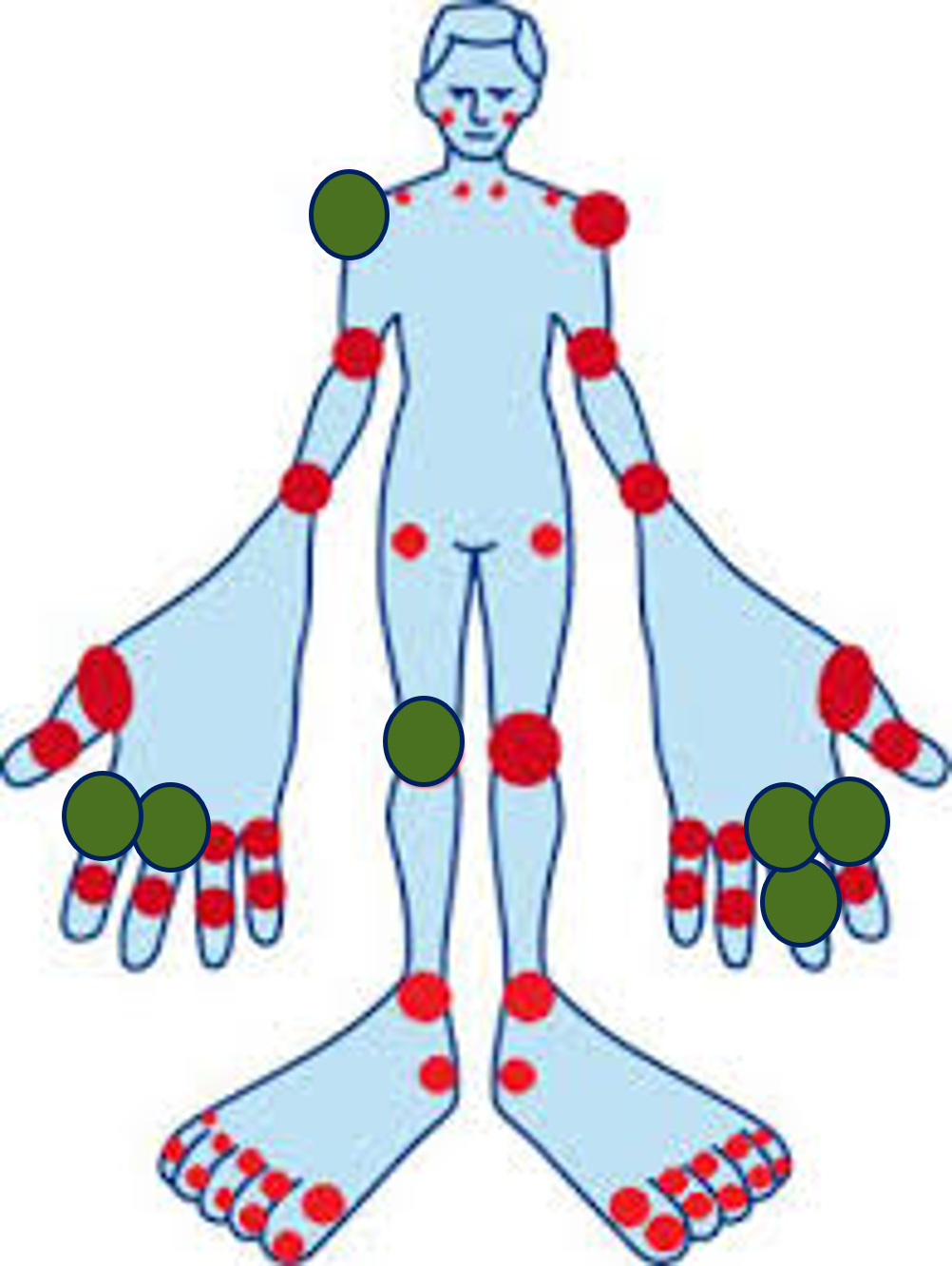
Figure 2: Pain sensitive joint 11/2019
Table 1: Laboratory findings 11/2019: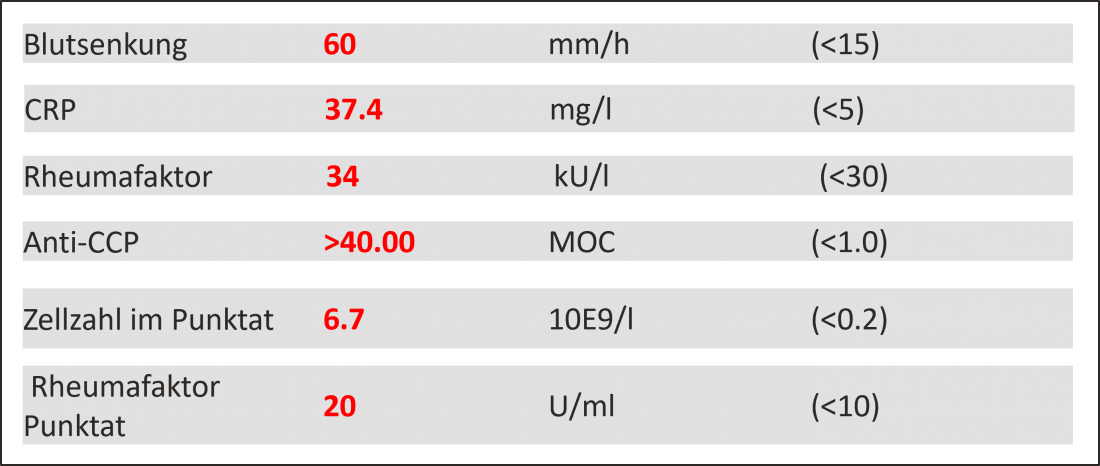
11/2019: Start of treatment with steroids and methotrexate.
- After the diagnosis of anti-CPP and rheumatoid factor-positive RA, the patient initially received 600 mg of ibuprofen plus a proton pump inhibitor (PPI) 3 times daily.
- In addition, his right knee was punctured (30 ml) and treatment with 20 mg peroral prednisolone (PDN) per day was started.
- One week later, the right knee joint was infiltrated with 40 mg of triamcinolone and baseline therapy was started with 15 mg of subcutaneous methotrexate (MTX) weekly plus 5 mg of folic acid weekly.
01/2020: Clinical and laboratory remission
- 2 months later, in January 2020, the patient achieved clinical and laboratory remission.
- The DAS28-CRP value of 2.06 indicated low disease activity.
- The CRP level had normalized to 2.0 mg/l and the erythrocyte sedimentation rate to 6 mm/h.
- Prednisolone was reduced to 10 mg/day in mid-December 2019 and to 5 mg/day starting in mid-January 2020.
03/2020: 1st relapse and treatment escalation with MTX and steroids.
- In March 2020, the patient suffered a recurrence with arthritis in the MCP joint III and PIP joint III of the left hand and right knee.
- DAS28-CRP had increased to 4.52, suggesting moderate disease activity.
- The CRP level had increased to 22.4 mg/l and the erythrocyte sedimentation rate to 42 mm/h.
- This was followed by a dose increase of subcutaneous MTX to 20 mg/week and oral PDN to 10 mg/day.
- In addition, the right knee joint was infiltrated with steroids for the 2nd time.
- Consequently, there was a marked improvement, and steroids were reduced to 5 mg/day within 2 months.
03/2021: 2nd relapse and initiation of treatment with upadacitinib.
- A little less than a year later, in March 2021, a 2nd relapse set in with arthritis in bilateral MCP joints II and III, PIP joint III of the left hand, and the right knee and elbow.
- The DAS28-CRP value of 5.43 suggested high disease activity.
- Laboratory testing revealed a CRP level of 22.3 mg/l and a blood sedimentation rate of 44 mm/h.
- To counteract the severe 2nd relapse, combination therapy of the oral JAK inhibitor upadacitinib (15 mg/day) plus PDN (10 mg/day) plus MTX (15 mg/week) was initiated.
06/2021: Achievement of remission
- 3 months after starting treatment with upadacitinib in combination with PDN and MTX, the patient achieved remission with a DAS28-CRP score of 1.94.
- The CRP level was 4.4 mg/l in June 2021, within the normal range, and the erythrocyte sedimentation rate was 32 mm/h.
- MTX dosing was then reduced by 2.5 mg per week every 4 weeks, and PDN was discontinued completely.
- Previously, the patient had interrupted both medications for 2 to 3 weeks at a time because of the Covid vaccine, without experiencing relapses.
Since 10/2021: Upadacitinib monotherapy.
- Since October 2021, the patient has been receiving monotherapy with upadacitinib 15 mg/day.
- By then, the CRP level had further decreased to 0.2 mg/l and the erythrocyte sedimentation rate had decreased to 12 mm/h. There was a slight increase in alanine aminotransferase (ALAT) levels to 63 U/l, but this was not a cause for concern.
Until 10/2022: Sustained remission
- At follow-up visits in February, June, and October 2022, the patient was still in clinical and laboratory remission and completely symptom-free. Low-dose prednisone was completely discontinued in June 2022.
- In October 2022, both the CRP value of 0.6 mg/l and the erythrocyte sedimentation rate of 10 mm/h were within the normal range. The ALAT value had also normalized to 29 U/l.
Comment by Ioannis Papadopoulos, MD:
“The patient had been suffering from severe RA with polyarthritis in the finger joints and right knee for several years, which severely limited him not only in his daily life but especially in his job as a service worker. The RA could not be brought under long-term control even with steroids and MTX, and the patient suffered repeated relapses after dose reduction of steroids despite interim improvements. Finally, in March 2021, treatment was initiated with the JAK inhibitor upadacitinib, taken once daily as a tablet. Just 3 months after induction of upadacitinib, the patient achieved remission. We were confident that we would be able to discontinue the steroid treatment and MTX, as this had previously been temporarily trialed due to the covid vaccine. To date, the patient is living symptom-free on upadacitinib monotherapy and has returned to full work. He appreciates the effective, steroid-free treatment with upadacitinib and shows good adherence to once-daily tablet intake.”
The references can be requested by professionals at medinfo.ch@abbvie.com.
Brief technical information RINVOQ®
This contribution was funded by AbbVie AG, Alte Steinhauserstrasse 14, 6330 Cham.
CH-RNQR-220114_12/2022










