
Lung carcinoma usually presents to the general practitioner as advanced disease with mostly nonspecific symptoms: As a silent preclinical lung finding, it must be specifically sought. Knowledge of the clinical presentation of the disease, its histopathology, and the anatomic prognostic classification (TNM system) of lung carcinoma facilitates its detection. A targeted, time-saving clarification is possible on an outpatient basis. It is based on interdisciplinary, international standards.
Lung cancer is common, and it causes the most deaths of all malignancies each year – in Switzerland as well as around the world. The well-known, terse saying in medicine: “What is frequent is frequent!” refers to two things: knowing about the frequent – and thinking about it. The classification and diagnosis of lung carcinoma discussed in this article provides structured cornerstones and points of note for the physician’s daily routine. Preventive efforts represent the most important medical action to reduce the leading cause of cancer death worldwide. By an overwhelming margin, the focus is on the successful efforts to persuade their own patients to give up smoking – and to accompany them in doing so.
The practicing physician encounters lung carcinoma from two aspects:
- As advanced disease with specific and especially nonspecific symptoms (Tab. 1).
- As a silent, preclinical pulmonary finding.
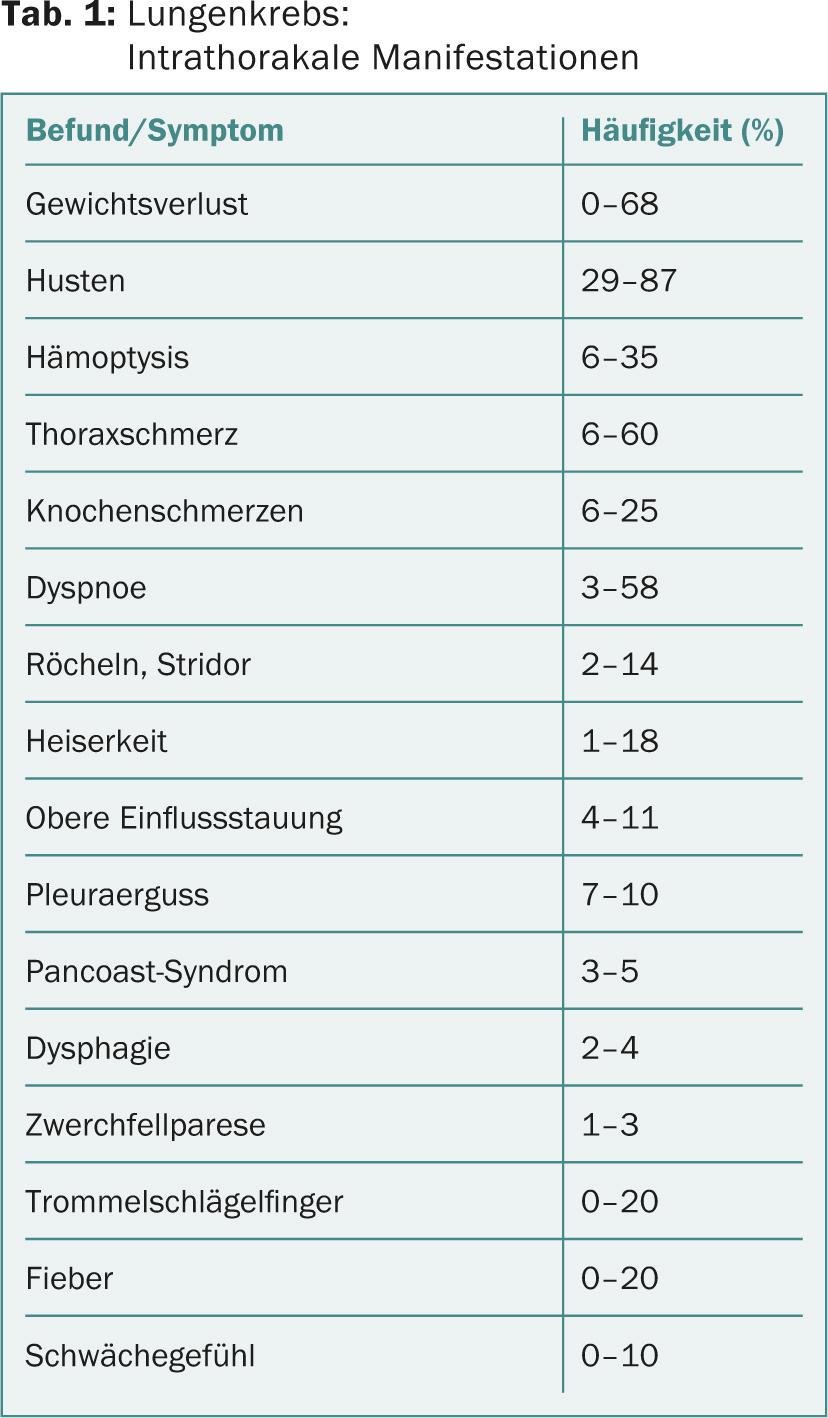
The symptomatic form of this disease dominates outpatient medical practice (approximately 90%). One-third each of the symptoms are produced by the primary site, by systemic signs such as anorexia, weight loss, asthenia, or already by signs of disease at the metastatic site. Unfortunately, the majority of these are already palliative situations. In contrast, clinically silent early carcinoma, if detected, is amenable to curative treatment. Any practical synopsis of lung cancer must take into account these two completely different starting points.
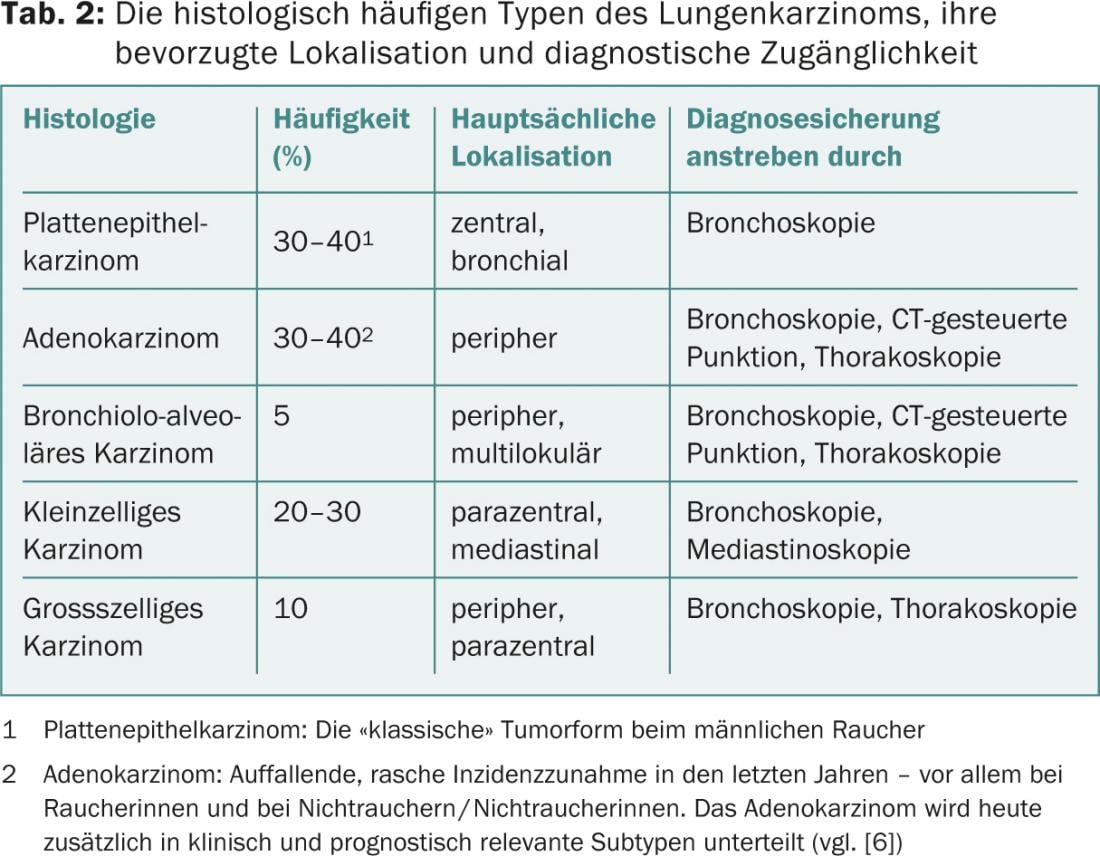
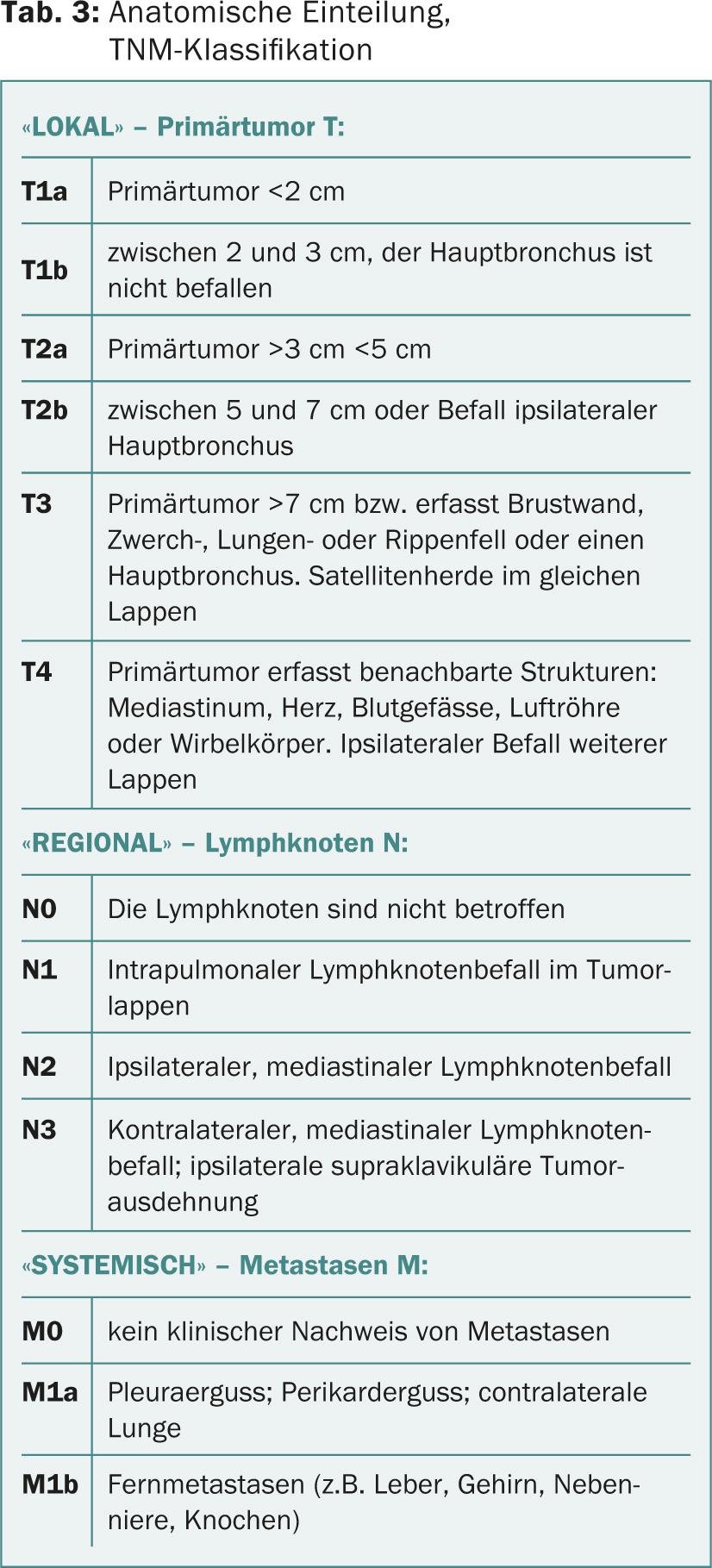
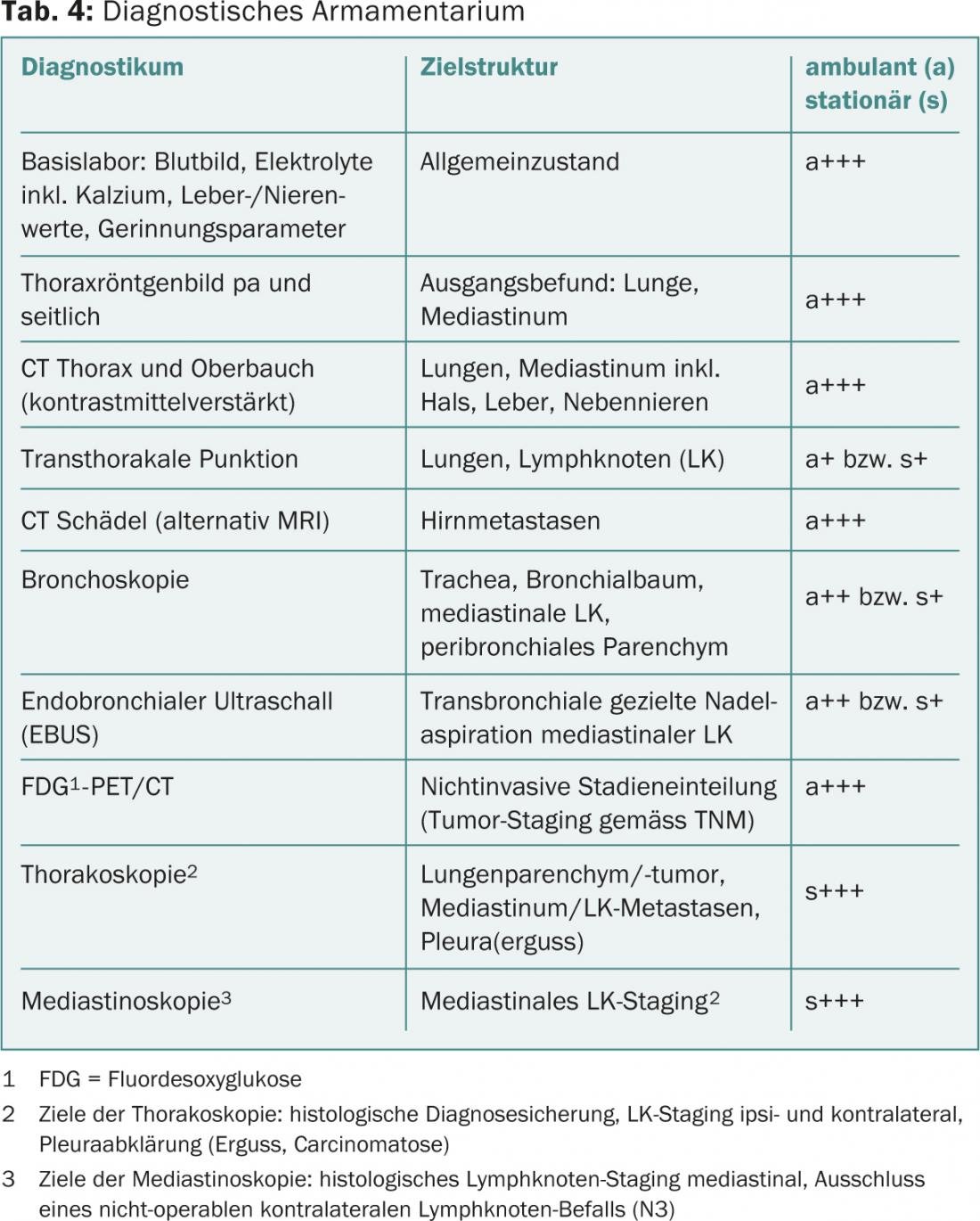
Knowledge of the histological (Tab. 2) and also the anatomical-prognostic classification (Tab. 3) of lung carcinoma as well as the diagnostic armamentarium (Tab. 4) enable a targeted, time-saving and economical detection and clarification cascade.
The symptomatic lung carcinoma
The majority of symptoms accompanying lung cancer are not specific (Table 1). It is therefore all the more important to relate these symptoms to the lung cancer profile of the patient concerned, i.e. to his possible risk factors. The greatest risks of developing lung cancer result from environmental factors:
- Smoking (85%) (10% of all smokers develop lung cancer!)
- Occupational exposure, e.g. to asbestos/arsenic/nickel (6-8%)
- Radon (5-7%)
- Ionizing radiation (2%)
- General air pollution (location dependent).
- Other important risk factors for developing lung cancer include:
- Age >50 years
- Upper/lower respiratory tract cancers (both personal and family history).
- Passive smoking (which per se causes a risk increase by a factor of 1.5 to 2.5).
If a majority of these factors apply, diagnostic conclusions are to be drawn from them, i.e., signs and findings obtained are to be weighted differentially as possible cancer manifestations. For example, the triad: nicotine abuse, COPD, and hemoptysis is worthy of clarification despite a negative chest x-ray.
Whether the further procedure can be ordered by the resident colleague and then performed on an outpatient basis is decided by the patient’s health condition. If respiratory failure, demonstrable hemoptysis, upper influence congestion, infectious septic signs, or accompanying neurologic symptoms exist, urgent hospitalization is indicated.
The outpatient clarification algorithm
If the patient’s clinical condition is stable, the algorithm in Figure 1 indicates the targeted approach.
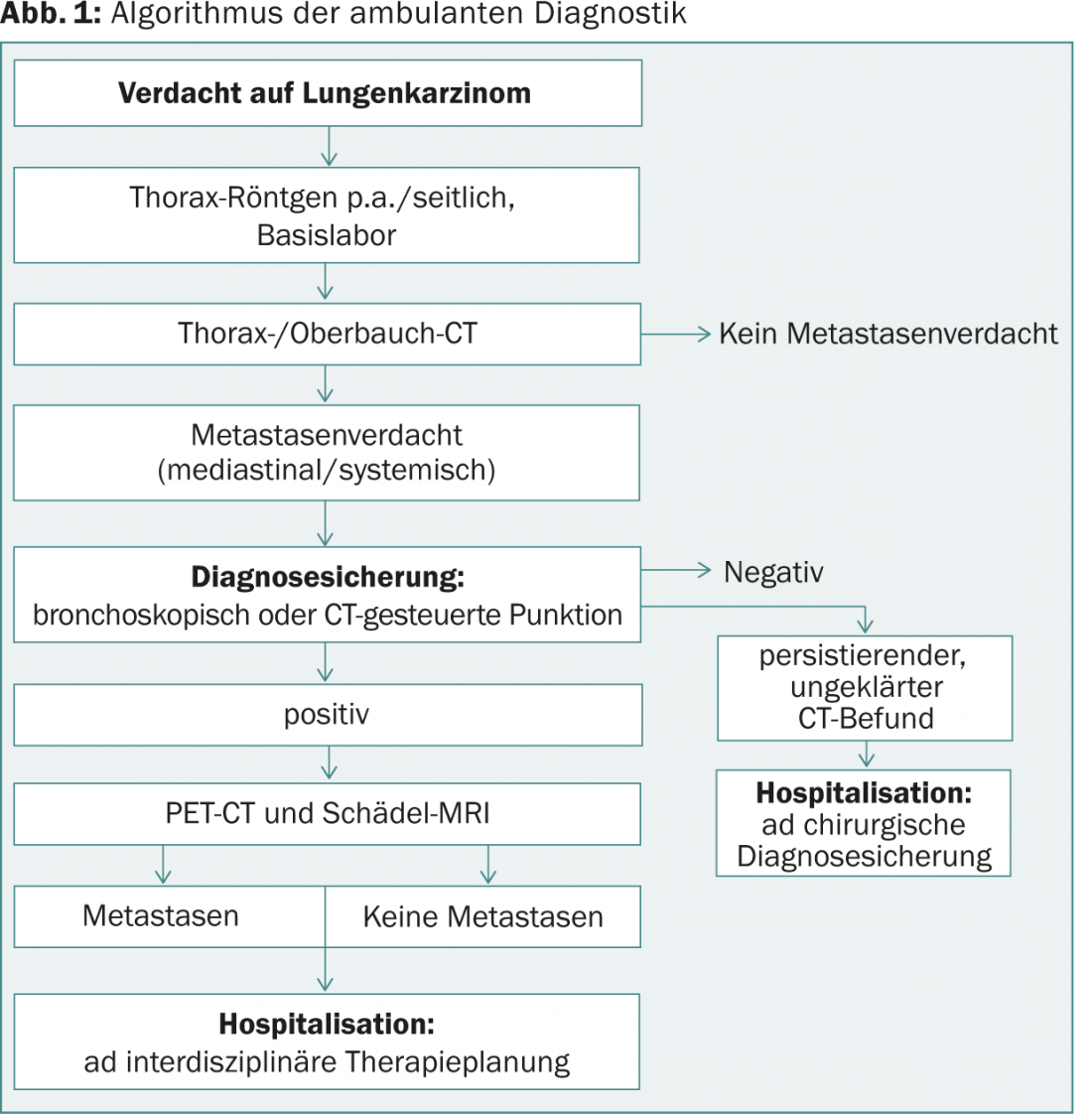
- Routine laboratory values are nonspecific in lung cancer or they refer to concomitant diseases such as poststenotic, pneumonic infiltrates, etc.
- Tumor markers (CRP, SCC, CEA, NSE, CYFRA 21-1, M2-PK) do not have a proven value in cancer screening, their sensitivity is between 20 and 30%.
- Chest computed tomography (CT) scan documents the location and extent of regional pathology, but says nothing about its etiology. If technically accessible, CT-guided, cytologic or histologic diagnostic confirmation can be attempted simultaneously.
- Bronchoscopy is a key investigation. It depicts the location and extent of airway involvement and is also used to obtain endo- and transbronchial tissue samples for histologic diagnosis. Together with an ultrasound probe (EBUS), bronchoscopy allows, in addition to primary tumor diagnosis with high accuracy, so-called mediastinal lymph node staging (sensitivity >90%).
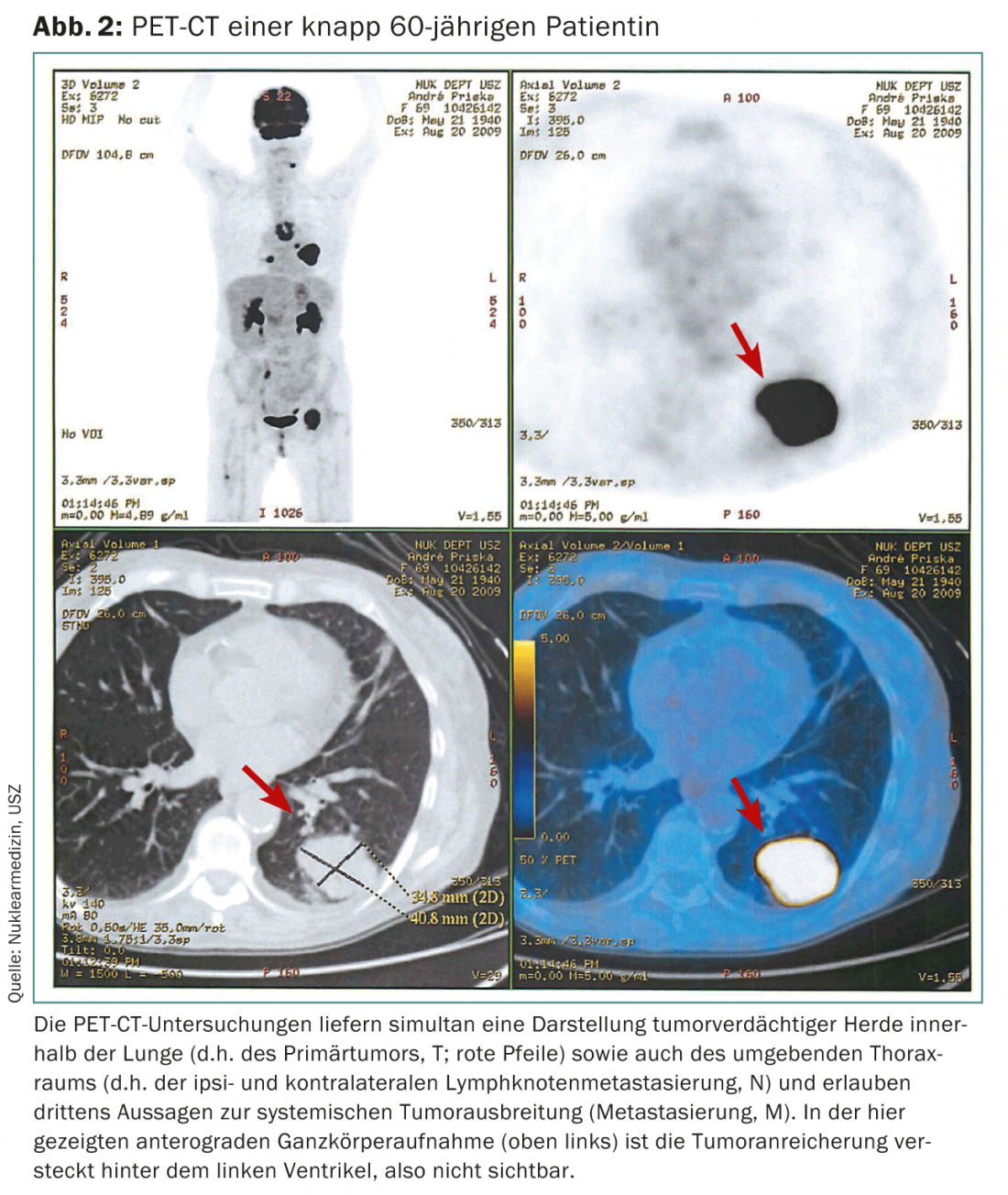
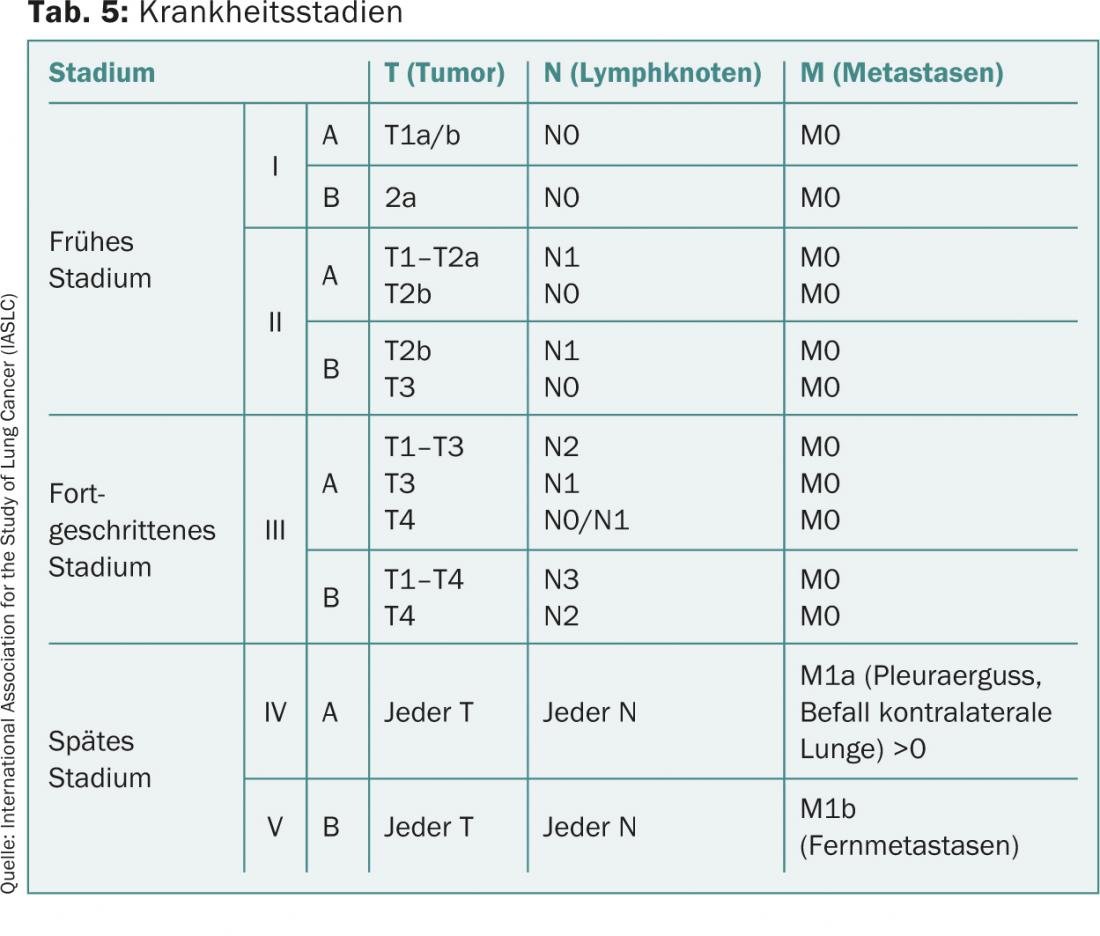
- If the diagnosis has been confirmed by then, the next step is positron emission tomography (PET) as whole-body tumor staging (Fig. 2). The PET is combined with a CT to better identify possible tumor sites. Thus, the local (T), regional (N), and systemic (S) data that are important for the further (M) tumor extent mapped (Tables 3 and 5).
- CT or MRI imaging of the skull is necessary to exclude brain metastases; PET is not suitable here because of the high glucose turnover in the brain.
Inpatient follow-up procedure in terms of therapy
Once the possible outpatient clarifications have been completed, the colleague’s active involvement in the practice ends. The further procedure must be performed on an inpatient basis and may include thoracoscopy or mediastinoscopy as a further diagnostic step. After completion of the internal clinic diagnostics, the further procedure is determined in the interdisciplinary tumor board (oncologists, radiotherapists, surgeons, pneumologists).
In disease stages with curative treatment intent (I to IIIb), the procedure follows the internationally established standards. In palliative stages (IIIb and IV), a patient- and symptom-specific approach is sought – taking into account currently ongoing studies. Due to the increasing experience with personalized medicine, new interdisciplinary treatment strategies are emerging, which allow curative approaches even in previously palliative stages in individual cases.
The asymptomatic lung carcinoma
If conventional chest radiographs were taken in two planes, for example, because of trauma or suspected pneumonia, the practicing physician is confronted with the finding of noncalcified pulmonary nodules in his patients. Differential diagnosis includes presymptomatic lung carcinoma. If this is the case, once the diagnosis has been made, the affected person should be counted among the 25% of lung cancer patients who can be given potentially curative surgical therapy. Here, the 5-year survival is between 25 and 85% depending on the stage of the disease. On conventional chest radiograph, parenchymal changes are visible from approximately 10 mm in diameter, unless obscured by bony structures or by the cardiac shadow.
The more peripheral they are in the parenchyma, the better they can be delineated from orthograde pulmonary vessels. The diagnostic approach to the unclear pulmonary focus is summarized in Figure 3.
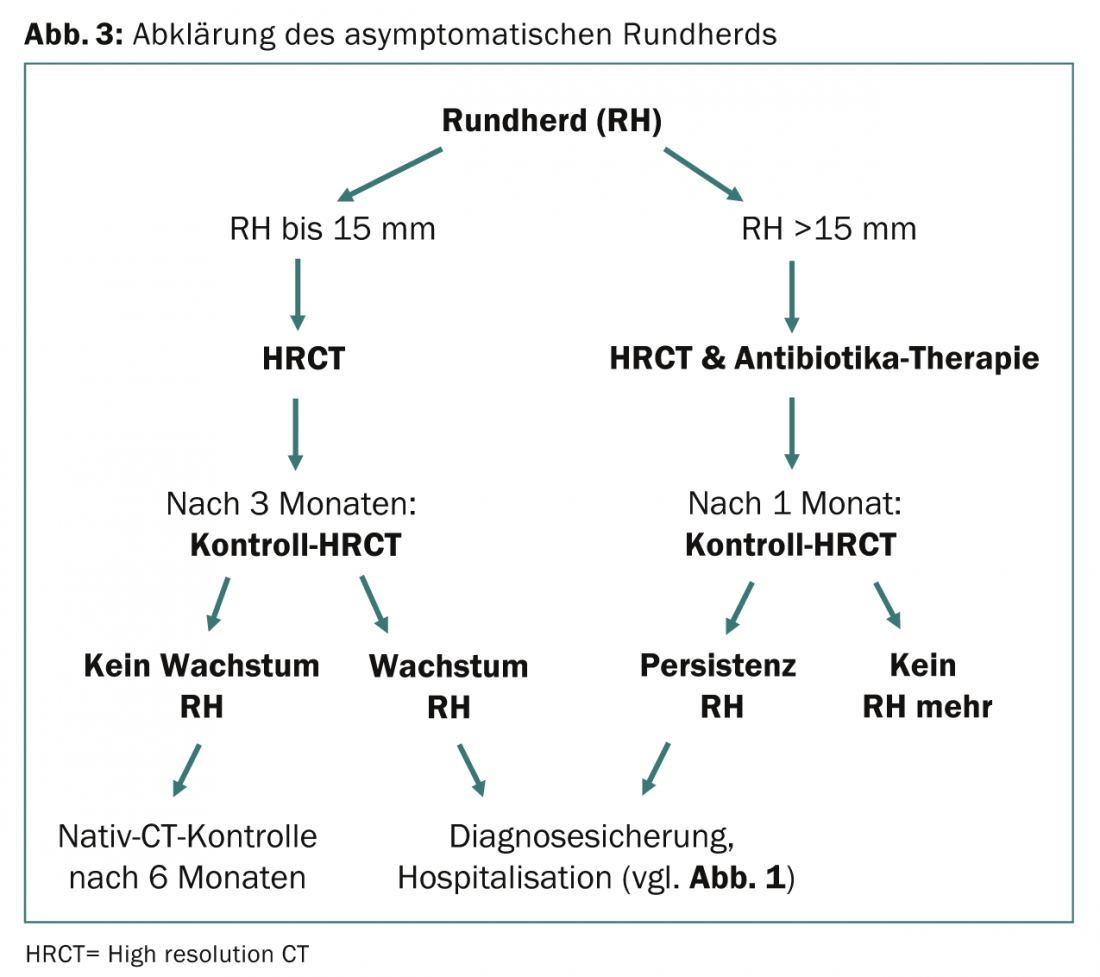
Noncalcified round foci up to 15 mm in diameter should be proven by computed tomography and rechecked by CT after three subsequent months. High-resolution CT is suitable for this purpose (no contrast medium required, thus economically much more favorable). If the findings increase in size, histological confirmation of the diagnosis is indicated.
If a round focus is larger than 15 mm in diameter, it may not be detectable on follow-up CT after one month under antibiotic therapy. Otherwise, the diagnosis must be forced. If carcinoma is positively detected, this is followed by an algorithm as shown in Figure 1.
CONCLUSION FOR PRACTICE
- Prophylactic medical intervention – smoking cessation – is by far the most successful approach to reducing lung cancer.
- Having the most structured knowledge possible about lung cancer facilitates differential diagnostic considerations in symptomatic patients as well as targeted case finding among high-risk patients.
- In principle, the diagnosis does not require inpatient clarification, provided that the lung carcinoma can be detected by computed tomography (cytology) or bronchoscopy (cytology, histology).
- PET-CT allows differentiated anatomical assignments and specifies and paves the way for further diagnostic procedures.
- In case of severe clinical symptoms and lack of cyto- or histological confirmation of the diagnosis, hospitalization becomes necessary.
Literature:
- Hopwood P, et al: Symptoms at presentation for treatment in patients with lung cancer: implications for the evaluation of palliative treatment. The Medical Research Council Lung Cancer Working Party. Br J Cancer 1995; 71: 633.
- Tanoue LT, et al: Lung Cancer: Epidemiology and Carcinogenesis. In: Shields TW, Locicero J, Ponn RB, Rusch VW (Ed): General Thoracic Surgery. Lippincott Williams & Wilkins 2005, 1425-1441.
- I-ELCAP: http://ICScreen.med.cornell.edu.
- National Lung Screening Trial by National Cancer Institute, USA: www.cancer.gov/NLST.
- Goeckenjan G, et al: Prevention, diagnosis, therapy and follow-up of lung cancer. Interdisciplinary S3 Guideline of the German Society of Pneumology and Respiratory Medicine and the German Cancer Society 2010.
- Yoshizawa A, et al: Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Modern Pathology 2011; 24: 653-664.
- Rami-Porta R, et al: The revised TNM staging system for lung cancer. Ann Thorac Cardiovasc Surg 2009; 15(1): 4-9.
InFo Oncology & Hematology 2013; 1(1): 10-15.









