
The results of the SPRINT study – lower mortality with more intensive hypertension treatment – were the focus of interest at the 11th Hypertension Day. However, it is not clear whether the blood pressure target values will be set lower again, because cost-benefit analyses are still pending. Other topics included the approach to refractory hypertension and setting targets in elderly and frail patients.
In his presentation, Prof. Frank Ruschitzka, MD, University Hospital Zurich, discussed the SPRINT study [1]. 9300 individuals with blood pressure above 130 mmHg and increased cardiovascular risk, but without diabetes, were randomized into two groups: Intensively treated patients were targeted to have systolic blood pressure (SBD) below 120 mmHg, and standard therapy patients were targeted to have SBD below 140 mmHg. After a median follow-up of 3.2 years, the study was terminated early because significantly fewer cardiovascular events occurred in the intensive therapy group (1.65% vs. 2.19% per year). All-cause mortality was also significantly lower in patients receiving intensive therapy. Side effects such as hypotension, syncope, electrolyte disturbances, and acute renal failure were more common in the intensive treatment group, but falls were equally common as in the standard treatment group.
The results of the SPRINT study will certainly be a talking point in the next discussion of blood pressure targets. There is no cost-benefit analysis yet. If the target values of the SPRINT study were to become general target values, a large part of the population would become hypertension patients (in need of treatment) at a stroke.
Plea for 24-hour measurement
High variability of blood pressure is dangerous, explained Prof. Gianfranco Parati, Milano (Italy): Individuals with highly variable blood pressure have a significantly increased risk of organ damage, such as stroke or cardiovascular events. The same applies to people whose blood pressure does not drop during the night (“non-dippers”). In order to eliminate diurnal variability as far as possible, drugs should be prescribed in such a way that, on the one hand, they do not act for only a few hours and, on the other hand, they are also adapted to the patient’s personal situation (e.g., in the case of “non-dippers” taking the antihypertensive in the evening).
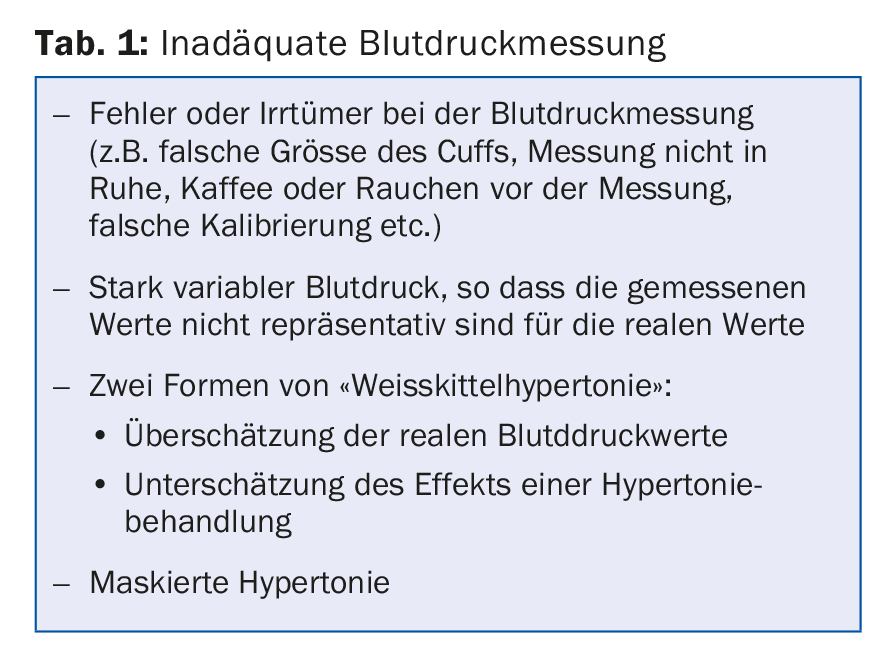
To eliminate errors in blood pressure measurement (Table 1) and to determine the variability of blood pressure, it is difficult to avoid 24-hour blood pressure measurement and ambulatory blood pressure measurements. “Measurements in practice show only the tip of the iceberg,” Prof. Parati reminded us.
Therapy-resistant hypertension – how to clarify?
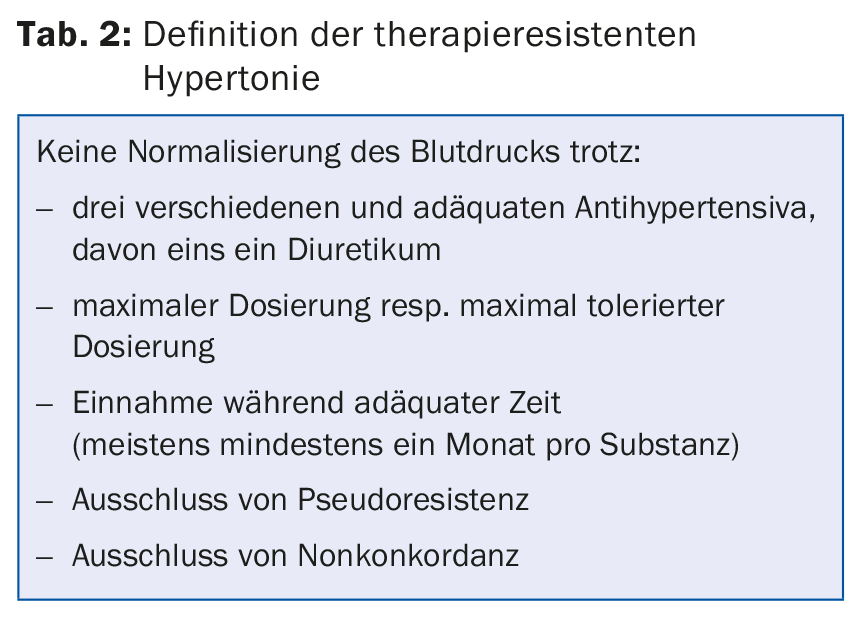
Several studies have shown that a single measurement of SBD in the office or hospital with values between 120 and 157 mmHg is not suitable to diagnose controlled or excessive blood pressure with sufficient certainty [2,3]. “So physicians are not very good at diagnosing hypertension in their practice,” emphasized Prof. Edouard Battegay, MD, University Hospital Zurich. “For this reason, 24-hour measurement is the gold standard.” The most reliable results come from a combination of office, home and 24-hour measurement. This is particularly true in patients with supposedly refractory hypertension (Table 2) : When a 24-hour measurement is performed at , blood pressure proves normal in one third of “therapy-resistant” patients.
Prof. Battegay recommended clarifying five questions when treatment resistance is suspected:
- Is the blood pressure permanently elevated?
- Are there additional risk factors?
- Is there end-organ damage?
- Has secondary hypertension been ruled out?
- What are the comorbidities? (Tab. 3)
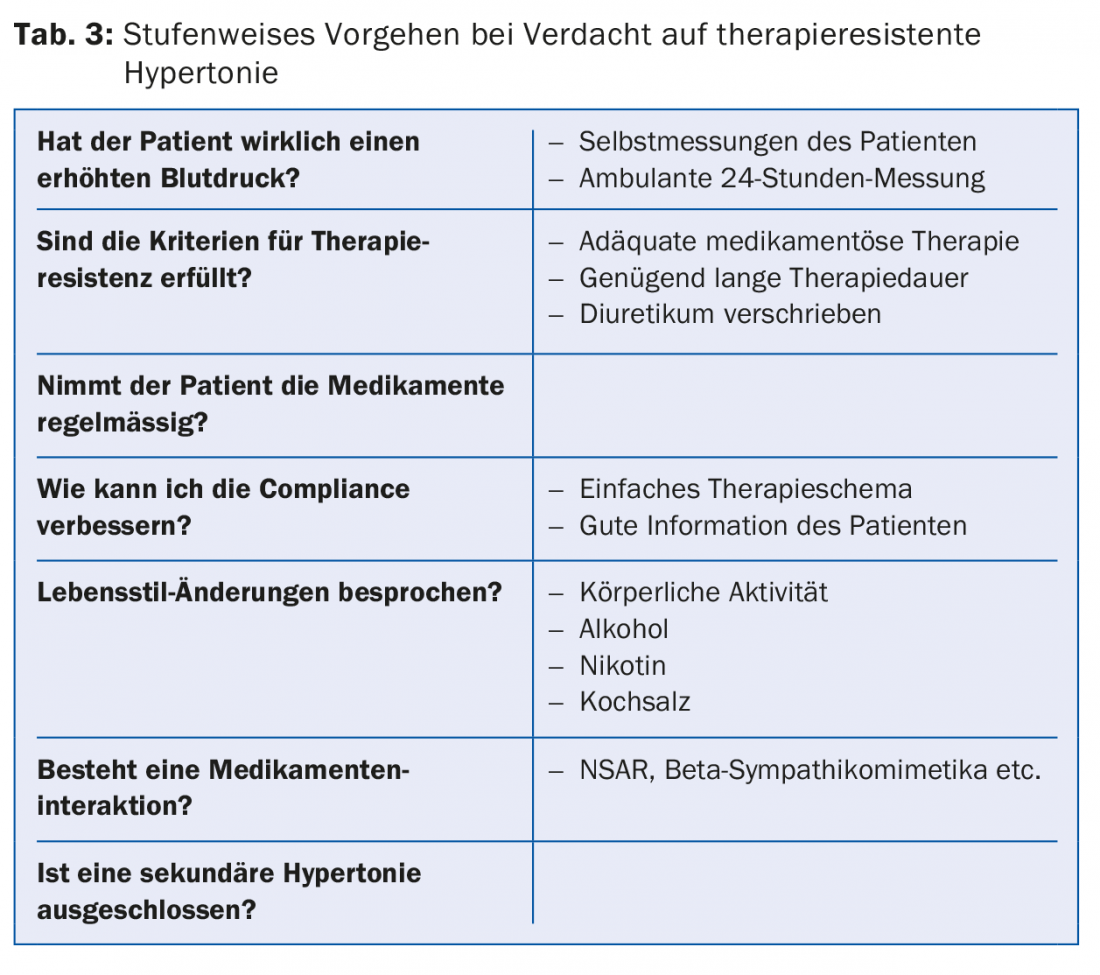
Risk factors for resistance to therapy: diabetes, NSAIDs, sleep apnea syndrome.
Patients with metabolic syndrome or diabetes have a higher incidence of treatment resistance. Because of the lack of “dipping,” at least one of the antihypertensives should be taken in the evening. Another risk factor for treatment resistance is obstructive sleep apnea syndrome. CPAP therapy not only improves sleep quality, but also lowers blood pressure levels – both at night and during the day. Non-steroidal anti-inflammatory drugs (NSAIDs), which are taken by many patients, can also increase blood pressure. “Unfortunately, there are no guidelines on how to proceed in such a situation,” Prof. Battegay said. “It’s a matter of making an individual decision.”
In case of real resistance to therapy, the drug regimen should first be optimized (adjustment diuretics, aldosterone antagonists). Alpha blockers, minoxidil, or centrally acting sympatholytics may be evaluated as second-line therapy.
Confusion in hypertension target values
Prof. Dr. med. Andreas Schönenberger, Geriatric University Hospital Bern, became somewhat nostalgic in his lecture: “Everything used to be much simpler, even the target values for hypertension.” In 2005, 140/90 mmHg applied to all resp. 130/80 mmHg for patients with diabetes or renal insufficiency. Today, there are a variety of guidelines, national and international, with different target values. “It’s a huge mess!”
With regard to the SPRINT study, the speaker noted that it mainly refers to rather fit seniors, as sicker seniors were not allowed to participate in the study at all. In daily practice, however, elderly people often have comorbidities that severely limit their life expectancy and/or quality of life, such as dementia. How low – if at all – should excessively high blood pressure be lowered in these individuals? The CRIME criteria provide practical recommendations in this regard [4]:
- In patients with dementia or marked functional limitations, strict blood pressure lowering (<140/90 mmHg) is not recommended.
- In patients with dementia or marked functional limitations, hypertension treatment with more than three antihypertensive agents should be avoided.
- In patients with a life expectancy of less than two years, strict blood pressure reduction (<140/90 mmHg) is not recommended.
- If falls occur as a result of orthostatic hypotension (or symptomatic orthostatic hypotension), the number of antihypertensive drugs should be reduced.
Individual target values in the elderly
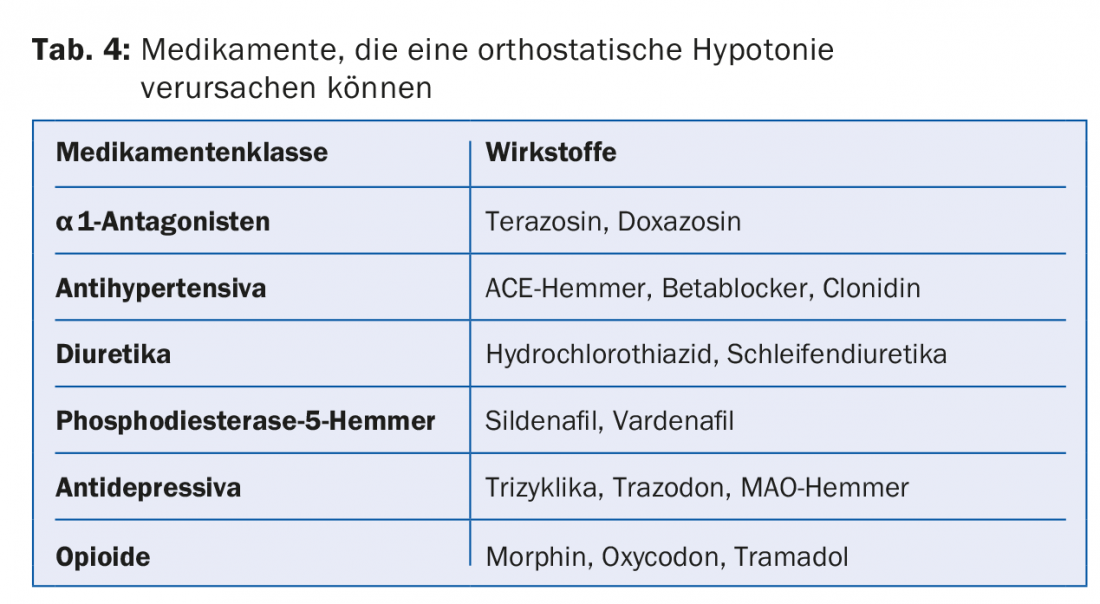
In practice, people often forget to diagnose cognitive impairment or dementia. However, this diagnosis is particularly important in determining the indication for hypertension therapy and target blood pressure levels. In addition, dementia can greatly affect compliance. “If blood pressure levels are lowered too much, there is a risk of orthostatic problems or decreased organ perfusion, which, in the case of the brain, can negatively affect cognition,” the speaker said. “Because of the simultaneous lowering of diastolic blood pressure, myocardial ischemia may also develop.” Orthostatic hypotension becomes more common with age, possibly caused by medications (Table 4). The orthostasis problem often results in the inability to achieve target blood pressure values.
However, advanced age alone is no reason to forgo good blood pressure control. Prof. Schönenberger presented a 90-year-old patient with a long list of diagnoses (apart from arterial hypertension, coronary heart disease, COPD, mild cognitive impairment, mild renal insufficiency, hypothyroidism, vitamin deficiency, among others) who had repeated falls. In this patient, it is worthwhile to keep blood pressure well controlled and minimize the risk of falls by expanding medication: “None of the patient’s diagnoses directly reduce life expectancy. At the same time, he is at very high risk for cardiovascular events or stroke. Such an event would be a double disaster because the patient is caring for his wife, who has dementia.”
Take-home-messages
- Blood pressure targets may be relaxed if life expectancy is expected to be less than one to two years, especially in advanced dementia.
- Target values should be determined individually in elderly patients, depending on biological age and drug tolerance.
- In fit older patients and with good tolerance of therapy, the same target values should be aimed for as in younger patients.
- Keep an eye on reduced perfusion of organs (brain, kidney, heart) and orthostatic hypotension and relax target values if necessary.
Source: 11th Zurich Hypertension Day, January 21, 2016, Zurich
Literature:
- SPRINT Research Group: A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med 2015 Nov; 373(22): 2103-2116.
- Hodgkinson J, et al: Relative effectiveness of clinic and home blood pressure monitoring compared with ambulatory blood pressure monitoring in diagnosis of hypertension: systematic review. BMJ 2011; 324: d3621.
- Powers BJ, et al: Measuring blood pressure for decision making and quality reporting: where and how many measures? Ann Intern Med 2011; 154: 781-788.
- Onder G, et al: Recommendations to prescribe in complex older adults: results of the CRIteria to assess appropriate Medication use among Elderly complex patients (CRIME) project. Drugs Aging 2014; 31(1): 33-45.
HAUSARZT PRAXIS 2016; 11(4): 37-39









