Nearly 4200 attendees registered at the DDG Fall Meeting 2021which was held under the motto “Diabetes and obesity – together through thick and thin” – was a complete success. The hybrid congress focused on current scientific, socio-political and psychological aspects of the widespread diseases diabetes mellitus and obesity. This includes the metabolic patient, who brings with him the risk of heart failure, among other things. What to do then?
The prevalence of heart failure is high and also steadily increasing. This also has implications for diabetology, as both heart failure and type 2 diabetes share common risk factors. These include age, family history, obesity, fat distribution, hypertension, and smoking. In addition, both are independent risk factors for the other disease. In diabetic patients, the risk of heart failure is two to three times higher. In addition, the likelihood of all-cause and cardiovascular mortality increases by 60-80% when both conditions are comorbid. In an observational study of patients with type 1 diabetes, the relationship between glucose control and the incidence of heart failure was clarified: Accordingly, a 1% increase in HbA1c is associated with a 30% increase in the incidence of heart failure. Accordingly, the prognosis of HFrEF or HFpEF worsens when diabetes is present.
Guideline recommendations up to date
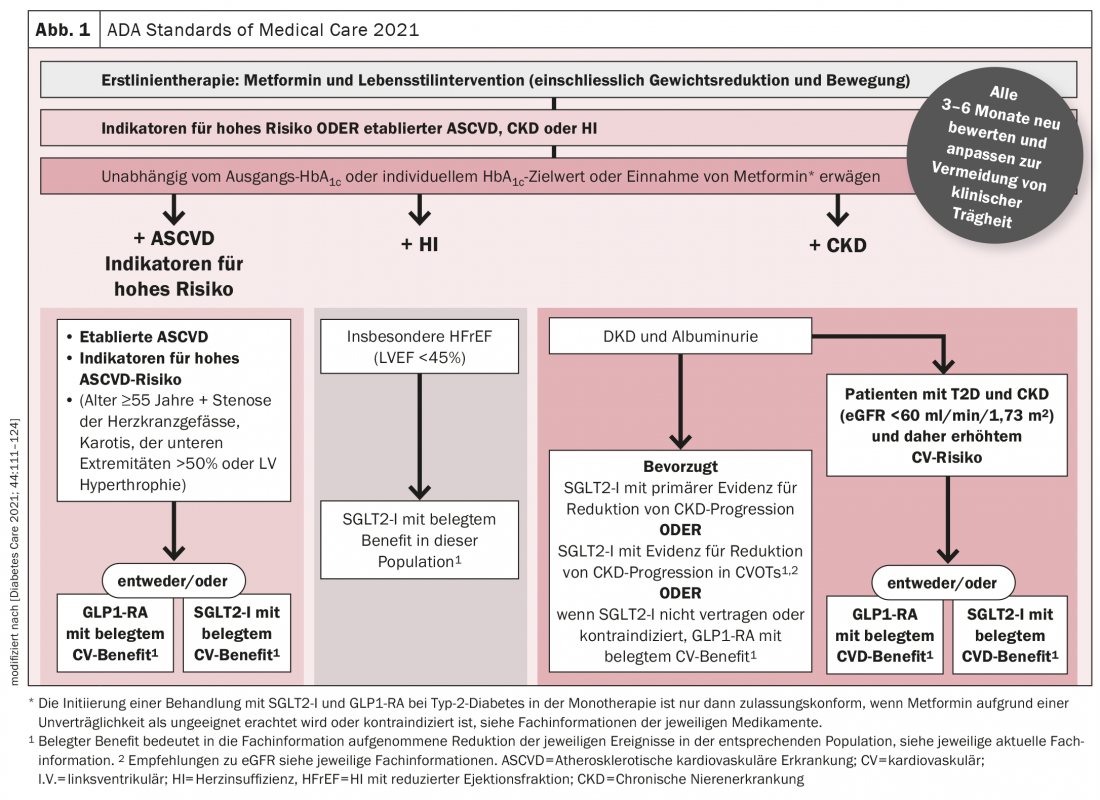
Therefore, a major focus is on effective treatment to improve prognosis and protect organs. The National Guideline on Type 2 Diabetes therefore recommends the use of SGLT2 inhibitors or GLP-1 receptor agonists for patients with high or very high cardio-renal risk. The current experience with the new substances led to a recommendation in the general approach to the choice of antidiabetic drugs (Fig. 1) . It is important to set the right course early.
The current heart failure guidelines also address this issue. Heart failure is classified into three phenotypes: HFrEF (LVEF ≤40%), HFmEF (LVEF 41-49%), and HFpEF (LVEF ≥50%). In the management of HFrEF, the four pillars of ACE-I/ARNI, BB, MRA, and SGLT2-I can be used. The order may vary.
Congress: DDG Fall Conference 2021
CARDIOVASC 2021; 20(4): 27 (published 1/12/21, ahead of print).









