
Venous leg ulcer (UCV) results from chronic overpressure in the venous system of the lower extremity. The correct diagnosis is made by a detailed anamnesis, clinical examination and additional instrumental diagnostics. The foundation of successful ulcer treatment is the reduction of ambulatory venous hypertension through surgical/interventional treatment of the underlying disease and compression therapy.
Among the differential diagnoses in patients with leg ulcers, venous leg ulcer (UCV) is the most common. According to the literature, approximately 50-70% of patients with leg ulcers suffer from causative chronic venous insufficiency (CVI) [1]. The prevalence for advanced CVI with UCV in the population is approximately 1-1.5%.
Origin of the UCV
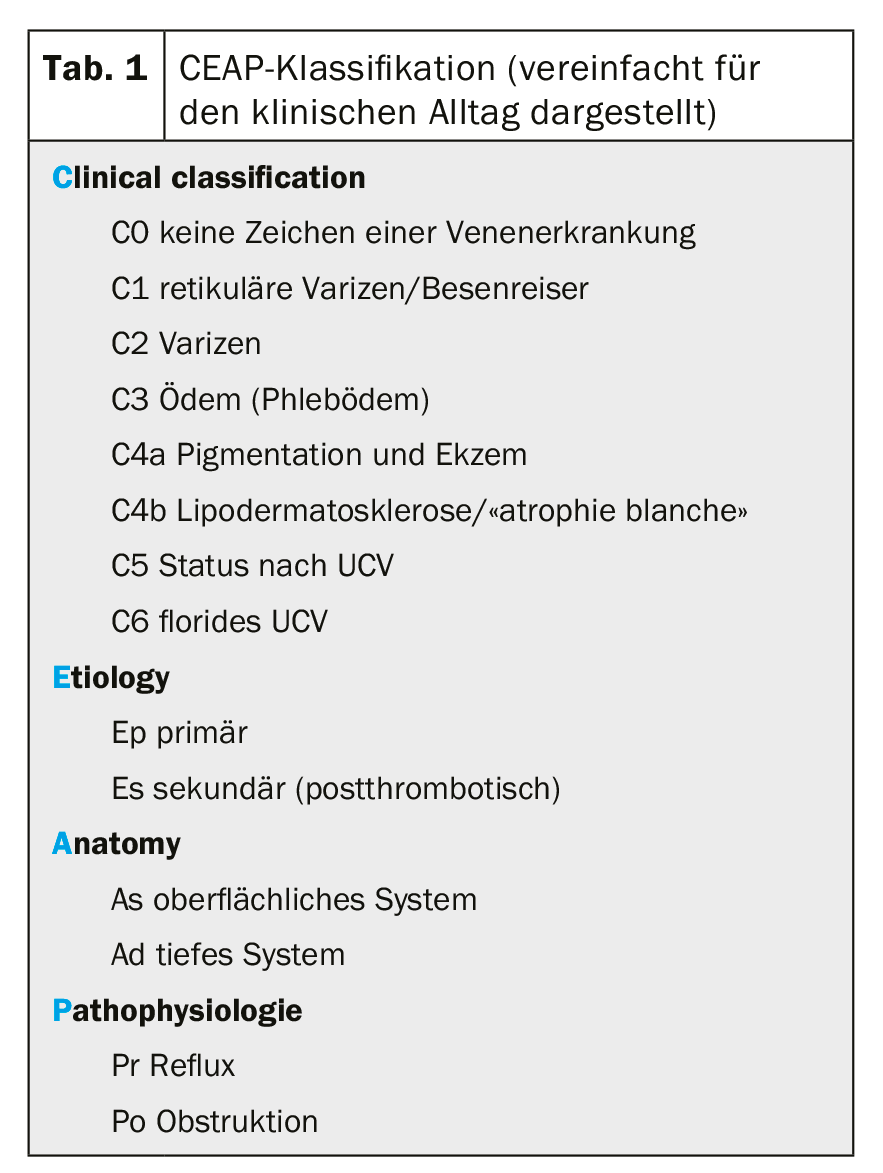
Underlying the development of chronic venous insufficiency is pathology in the superficial and/or deep venous system. While reflux in the superficial venous system (in the narrower sense of varicosis) leads only slowly to the development of higher-grade CVI (CEAP 4-6, Table 1) , functional and usually secondary disorders in the deep venous system (postthrombotic syndrome) lead much more rapidly to the clinical manifestation of CVI [2]. Both pathophysiological sequelae, reflux and obstruction, are culprits in venous hypertension In this context, persistent obstruction favors the development of CVI. In this context, one also speaks of ambulatory venous hypertension, meaning that venous pressure does not decrease even during exercise, i.e., the various pumping and suction mechanisms that serve to return venous blood and thus lower the pressure in the veins are reduced or no longer effective (calf muscle pump, squeezing of the plantar plexus, respiratory and cardiac suction phenomena, etc.) [3]. Fluid and protein leakage from the capillaries, complex inflammatory processes and the corresponding accumulation of specific inflammatory cells (macrophages and monocytes) result in a breakdown of the physiological skin and subcutaneous supply of nutrients and oxygen [4].
Clinic
UCV varies in pain depending on its location and not infrequently results from an initial minor injury to the skin. Ambulatory hypertension, accompanied by the metabolic changes described above, leads to itching that sufferers attempt to relieve with scratching, thereby violating skin integrity. Typically, the ulcers are found in the so-called gaiter zone, i.e. proximal to the malleolar plane, somewhat clustered medially. The integument shows the typical signs of long-standing venous congestion with ocher-colored areas (“purpura dermite jaune d’ocre”) and whitish, sclerosed areas (“atrophie blanche”).
The lesions, which are only small at the beginning, can become larger very quickly. Numerous home remedies have an unfavorable effect on the course. Extracts from plants or alcohol wraps further destabilize the skin and the wound edge, intensify the inflammatory processes and can lead to allergic reactions. The severity of the inflammation finds clinical expression in the amount of exudate. Ulcers with a high bacterial load also exude more fluid. Often, severe exudation is more decisive for the loss of quality of life than the local pain problem.
Diagnosis
Because the development of chronic venous insufficiency takes place over a long period of time, there are usually clear indications in the patient’s medical history. In the foreground is the question of previous venous thrombosis and previous interventions on the superficial venous system as an expression of superficial venous insufficiency. Those affected do not always remember a thrombotic event or it went unnoticed. If the history and clinical presentation of the ulcer support the suspicion of UCV, further phlebologic workup is performed with the goal of balancing the causative phlebologic pathology/pathophysiology. The gold standard for the examination of the venous system is color-coded duplex sonography (FKDS). the compression sonography. The cw Doppler examination alone can confirm the suspicion of venous disease and allows standard treatment (compression, wound treatment) to be carried out. Duplex sonography is required to plan causal phlebologic therapy [5,6]. In the case of ulcerations that have been present for years, a possible degeneration should always be considered and biopsy should be performed to exclude it.
Therapy
Because UCV results from ambulatory venous hypertension, the primary causative therapeutic approach is to counteract this venous hypertension. This is done conservatively by prescribing adequate compression. How much compression is “adequate” is a matter of controversy. It is still true that at least a well-fitting compression stocking of compression class II (23-32 mmHg) should be worn. Recent studies show that even compression stockings with a lower contact pressure can achieve a sufficient effect. It should be remembered that concomitant severe restriction of arterial blood flow (PAVK) must be excluded, especially in elderly patients. With palpable foot pulses, an ABI of >0.8, and no clinical signs of arterial circulatory dysfunction, compression therapy is feasible without additional angiologic evaluation.
The invasive treatment option focuses on surgical/interventional therapy for venous hypertension. Whether treatment of venous insufficiency accelerates healing of florid UCV is not clear. In contrast, elimination of insufficient epifascial veins significantly decreases the development of recurrent ulcer. Treatment options on the superficial venous system to eliminate the recirculation circuit are selected according to the findings (classical surgery, endoluminal thermal ablation, sclerotherapy). Therapeutic options on the deep venous system are less established and require careful and strict indication (endophlebectomy, valve reconstruction, valve transposition).
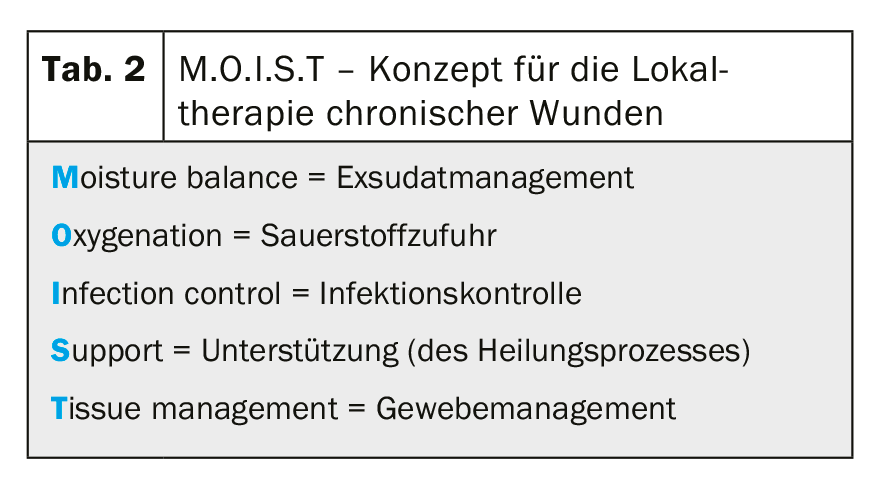
Local therapy is based on proven concepts for the treatment of chronic wounds. After measuring and documenting the wound and wound condition in as standardized a manner as possible, local treatment should be guided by a systematic approach. In addition to the long-established “TIME” concept [7], the “MOIST” concept [8] has been further developed to include the additional attributes “oxygenation” and “support” (tab 2) . In cases of clinical suspicion of a local infection, microbiological examinations are aimed at identifying the pathogenic germs. A correctly performed smear test can lead to usable results, but is inferior to wound biopsy in terms of informative value [9].
Instead of topical antibiotics, local antiseptics and, in case of evidence of infection, systemic antibiotic therapy are preferable. Empirical use of a broad-spectrum antibiotic has been shown to be effective in clinically manifest infection, in the author’s opinion, even in the absence of pathogen detection.
Depending on the assessment of the amount of exudate, highly absorbent dressings are applied or, if the wound situation is too dry, additional moisture is applied to the wound area. The amount of exudate and correct exudate management can always be inferred from the old dressing and the degree of maceration in the wound margin area.
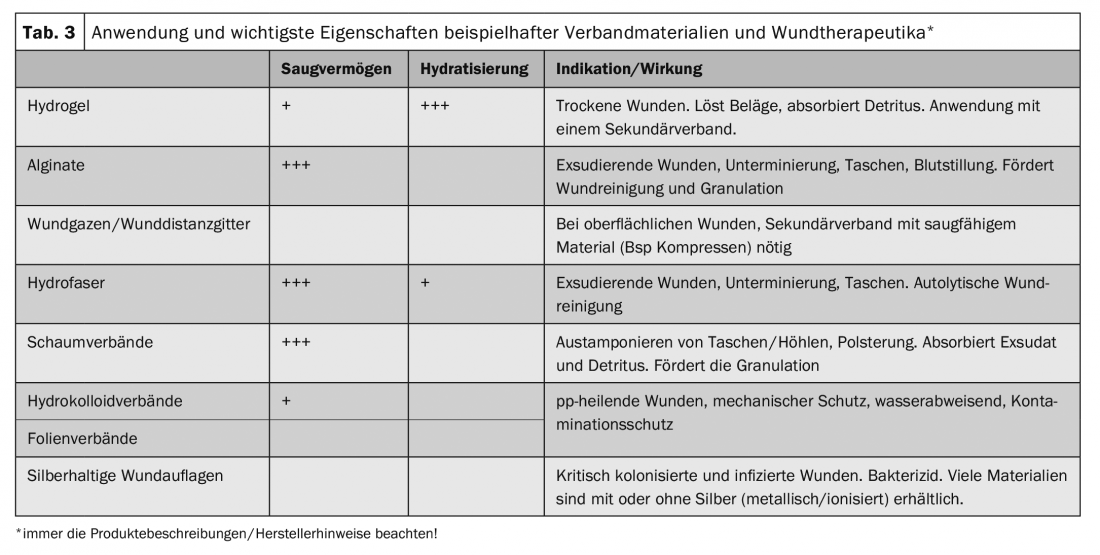
Cleaning and debridement of the wound bed is performed prior to reapplication of the wound dressing [10]. The dressing must be applied in such a way that the wound edge is optimally protected against maceration and excess wound secretion can be collected in the secondary dressing [11]. Non-adhesive and permeable wound dressings in the form of fatty gauzes, silicone dressings, etc. (so-called wound spacers) as well as semi-occlusive film dressings are suitable as primary dressings. If wound visits reveal excessively wet dressings, the frequency of dressing changes and the absorption capacity should be increased by adjusting the secondary dressing (Table 3).
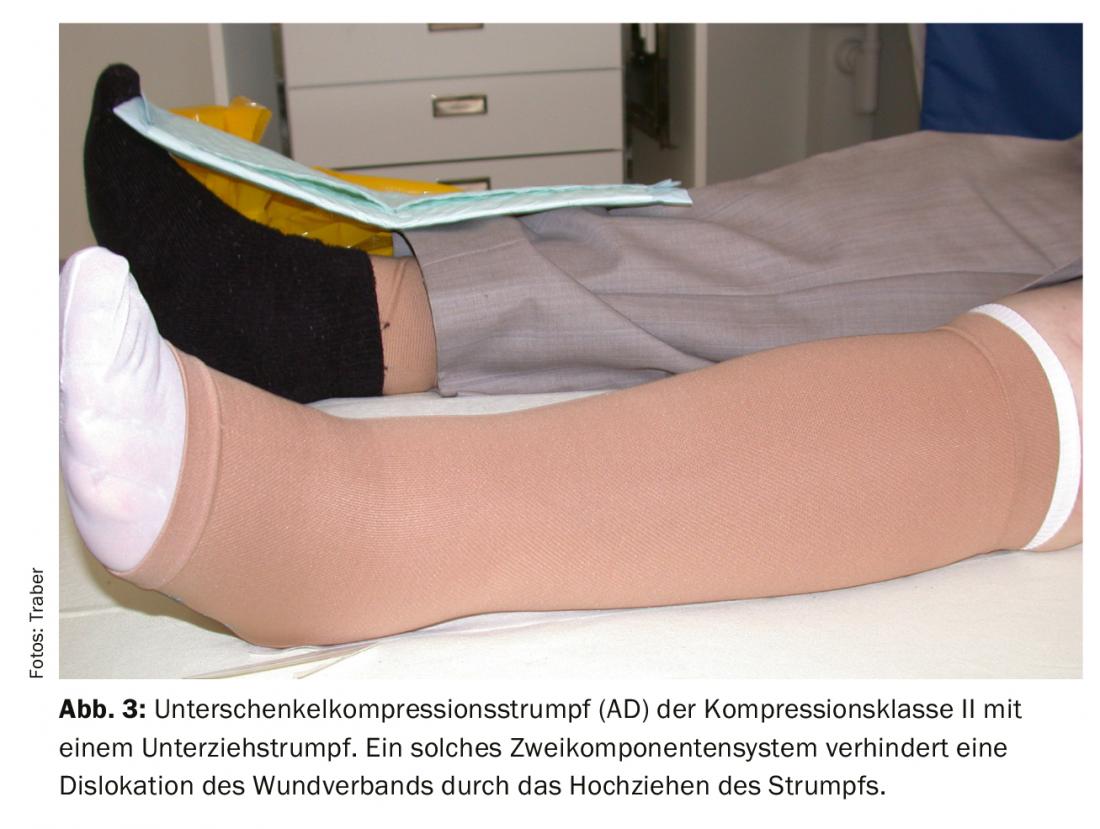
To ensure that the dressings remain in the intended position, a thin understocking can be used under the compression stocking. With the therapeutic goal of “ulcer healing”, a lower leg stocking (AD) is usually sufficient. In practice, in connection with local wound treatment, multi-layer well-padded compression therapy is preferable at the beginning. This ensures optimal decongestion and the persistence of locally applied dressings. To achieve a high working pressure, short-stretch bandages should be chosen and patients should be encouraged to move as much as possible to maximize the compression effect.



Therapy goals
Compression therapy is intended to reduce edema. This also reduces the inflammatory reactions with the result that the wound edge and wound bed experience a significant calming already in the first few days. This sedation is manifested by a decrease in pain and a reduction in the amount of exudate. If, at the same time, it is possible to create a wound climate that complies with the principles of modern moist wound treatment by applying appropriate wound dressings, UCV usually heals. However, experience shows that even with an optimal therapy strategy, a lot of time and patience must be invested.
Reconsideration and, if necessary, adjustment of the treatment or diagnosis is necessary if healing stagnates or if the clinical situation worsens. If healing stagnates despite verified diagnosis and therapy adjustments, supportive measures (use of specific wound therapeutics) should be considered. Local surgical measures such as extensive surgical debridement, ulcer shaving or ulcer excision, and defect coverage with skin substitutes or skin grafting must also be considered if healing does not progress.
If the clinical situation allows and the general condition of the patient permits a major procedure, repair of the phlebopathologic condition is also conceivable during the same procedure or during the same hospitalization.
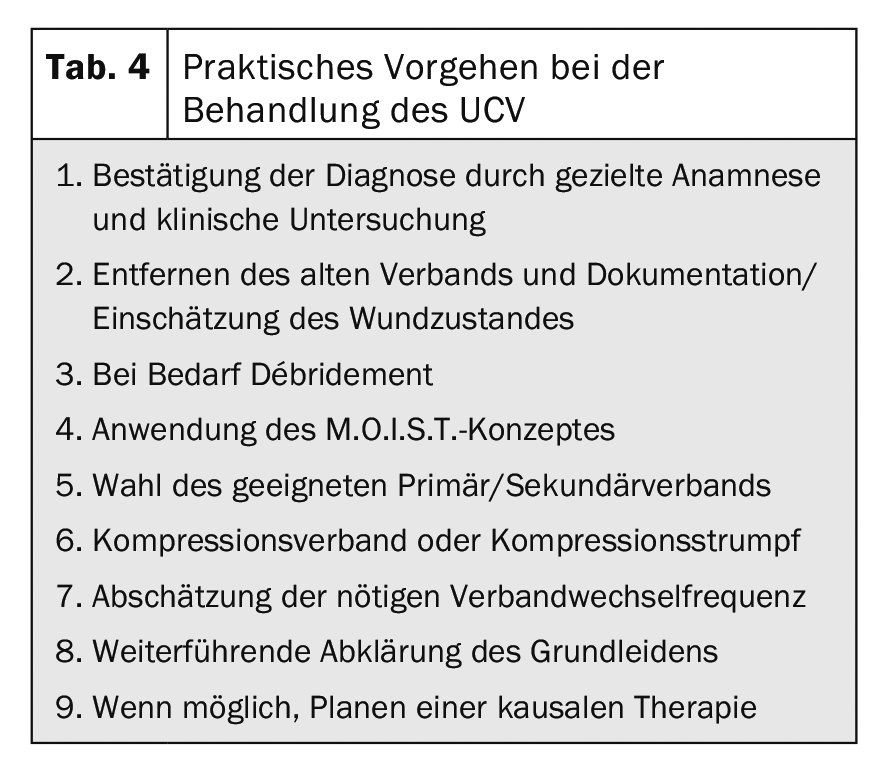
Table 4 summarizes again the practical procedure for the treatment of UCV.
Take-Home Messages
- UCV results from chronic excess pressure in the venous system of the lower extremity (venous hypertension). The correct diagnosis is made by a detailed anamnesis, clinical examination and additional instrumental diagnostics. The foundation of successful ulcer treatment is the reduction of ambulatory venous hypertension through surgical/interventional treatment of the underlying disease and compression therapy.
- Local therapy includes phase-adapted wound treatment (by choosing appropriate dressings adapted to the healing stage), regular debridement of the wound, and local infection treatment if there are appropriate signs of infection.
- In the absence of successful healing and verification of correct diagnosis, a surgical approach with extensive debridement/ulcer excision may be appropriate as a forward strategy.
- Surgical/interventional therapy of the superficial phlebopathology underlying the ulcer should be sought whenever possible.
- Permanent compression therapy should be considered depending on the phlebopathological findings and the greatest attention should be paid to skin care.
Literature:
- Tatsioni A, et al: Usual care in the management of chronic wounds: A review of the recent literature. J Am Coll Surg 2007; 205: 617-624.
- Labropoulos N, et al: Secondary chronic venous disease progresses faster than primary. J Vasc Surg 2009; 49: 704-710.
- Eberhardt RT, Raffetto JD: Chronic venous insufficiency. Circulation 2005; 111: 2398-2409.
- Raffetto JD: Inflammation in chronic venous ulcers. Phlebology 2013; 28(Suppl 1): 61-67.
- Rautio T, et al: Accuracy of hand-held Doppler in planning the operation for primary varicose veins. Eur J Vasc Endovasc Surg 2002; 24: 450-455.
- Haenen JH, et al. Venous duplex scanning of the leg: range, variability and reproducibility. Clin Sci 1999; 96: 271-277.
- Schultz GS, Barillo DJ, Mozingo DW, Chin GA: Wound Bed Advisory Board Members. Wound bed preparation and a brief history of time. Int Wound J 2004; 1: 19-32
- Dissemond J, Assenheimer B, Gerber V et al. M.O.I.S.T. – a concept for the local therapy of chronic wounds. J Dtsch Dermatol Ges 2017; 15: 443-445.
- Rhoads DD, et al. Comparison of culture and molecular identification of bacteria in chronic wounds. Int J Mol Sci 2012; 13: 2535-2550.
- Williams D, et al. Effect of sharp debridement using curette on recalcitrant nonhealing venous leg ulcers: A concurrently controlled, prospective cohort study. Wound Repair Regen 2005; 13: 131-137.
- Trengove NJ, et al. Analysis of the acute and chronic wound environments: The role of proteases and their inhibitors. Wound Rep Regen 1999; 7: 442-452.
DERMATOLOGY PRACTICE 2020; 30(2): 10-13









