The market approval of checkpoint inhibitors has sustainably improved the options for melanoma treatment. Impressive survival rates have been achieved in long-term studies. Although there are still many open questions, such as the management of side effects, modern immunotherapeutics are among the hopeful candidates for the treatment of black skin cancer.
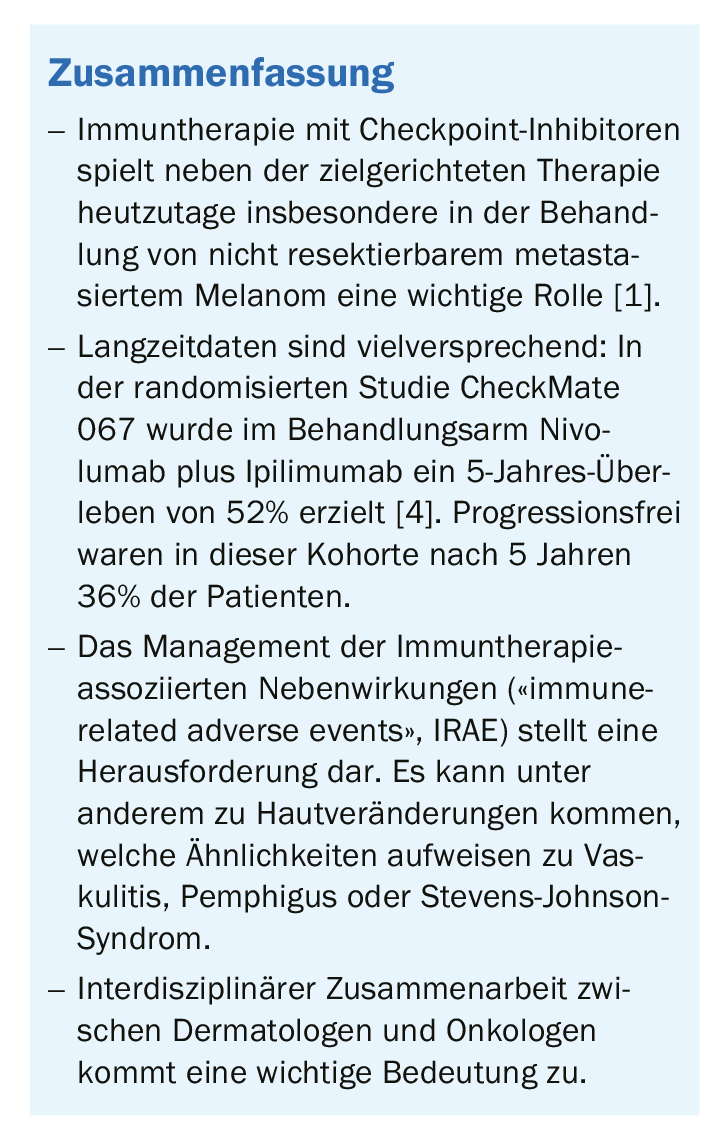
Especially in the treatment of non-resectable metastatic melanoma, immunotherapy now plays an important role alongside targeted therapy (BRAF and MEK inhibitors, among others) [1]. The spectrum of approved immunotherapeutics is continuously expanding. In Switzerland, the following checkpoint inhibitors are currently approved for melanoma treatment [2,3]: Ipiliumumab (Yervoy®), which belongs to CTLA-4, and the PD1 inhibitors nivolumab (Opdivo®) and pembrolizumab (Keytruda®). By counteracting the deactivation of the immune system, checkpoint inhibitors allow immune cells to attack the tumor again.
High 5-year survival rates in long-term study
The results of the CheckMate 067 randomized trial in patients with metastatic melanoma are promising [4]. Study participants were assigned to the following three treatment arms: Combination nivolumab plus ipilimumab or nivolumab treatment alone or ipilimumab monotherapy. In the past, these checkpoint inhibitors resulted in impressive remission rates and long-lasting remission. In this study, this trend was confirmed after 5 years in the cohort receiving the combination of nivolumab plus ipilimumab: A 5-year survival of 52% was achieved. This proportion was 44% in the nivolumab condition and 26% under ipilimumab. Progression-free in the nivolumab/ipilimumab cohort was 36% of patients after 5 years. The success of these therapies is somewhat overshadowed by their relatively high toxicity – in this study, for example, just over half of the patients in the nivolumab/ ipilimumab condition also experienced grade 3 and 4 adverse events [4].
The efficacy of ipilimumab was demonstrated years ago in a study involving nearly 700 patients with advanced black skin cancer [5]. Although the therapeutic results were promising, the proportion of those who did not respond to treatment was about 25% [5]. In particular, there are high hopes for the newer checkpoint inhibitors that target the surface molecule PD-1. Inhibition of the PD-1 pathway also promotes cancer cell targeting but appears to have slightly less dangerous side effects than CTLA-4, and a 2012 study with the PD-1 inhibitor nivolumab was encouraging [6]. About a quarter of patients with advanced skin cancer responded to treatment.
Management of side effects is a challenge
The expansion of indications has been accompanied by an increase in patients with immunotherapy-associated adverse events (“IRAE”) [7]. These are different from chemotherapy-related side effects. Thus, alopecia, vomiting, blood count changes, and infections are rare, but various autoimmune phenomena may occur [7]. Therefore, oncologic patients who exhibit new symptoms of this type should be contacted by their treating oncologist. If necessary, immunotherapy should be paused , and in case of severe and unexpected side effects, a report should be made to the pharmacovigilance center [7]. The severity of IRAE and associated implications for the further course of therapy is assessed using the Common Terminology Criteria for Adverse Events (CTCAE), which classifies IRAE into mild (grades 1-2), moderate (grades 3) and heavy (grade 4) Provides for side effects [8–10]. IRAE can lead to various skin lesions resembling classic dermatologic disease patterns (e.g., vasculitis, pemphigus, Stevens-Johnson syndrome) and cause an exacerbation of preexisting autoimmune skin disease. In exacerbations of psoriasis, the problem is that therapy with the anti-interleukin-17 antibody secukinumab, although effective, is probably associated with loss of tumor response [11].
Literature:
- Olah J: Update on immunotherapy in metastatic melanoma. Prof. Dr. Judit Olah, Review and Updates, Melanoma, EADV Congress, Madrid, Oct. 11, 2019.
- Swissmedic, www.swissmedic.ch
- Swiss Drug Compendium, https://compendium.ch
- Larkin JMG, et al: 5-year survival outcomes of the CheckMate 067 phase III trial of nivolumab plus ipilimumab (NIVO1IPI) combination therapy in advanced melanoma, Annals of Oncology 2019; 30: Supplement 5, www.annalsofoncology.org
- Hodi FS, et al: Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010; 363(8): 711-723.
- Topalian SL, et al: Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 2012; 366(26): 2443-2454.
- Gautschi O, et al: Update 2019: side effects of oncological immunotherapies, Swiss Med Forum 2019; 19(0910): 159-163.
- Haanen JBAG; ESMO Guidelines Committee. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2017; 28(Suppl4): iv119-iv142.
- Brahmer JR, et al; National Comprehensive Cancer Network. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol 2018; 36(17): 1714-1768.
- Postow MA, Sidlow R, Hellmann MD: Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N Engl J Med 2018; 378(2): 158-168.
- Esfahani K, Miller WH Jr: Reversal of Autoimmune Toxicity and Loss of Tumor Response by Interleukin-17 Blockade. N Engl J Med 2017; 376(20): 1989-1991.
DERMATOLOGY PRACTICE 2020; 30(2): 32