
The www.swissheart-coach.ch program is designed to help health-conscious individuals and patients manage cardiovascular risk factors in the prevention and management of disease. The program can also be an aid for professionals in accompanying and counseling those affected. The “Swissheart-Coach” is unique in that it includes all known risk factors. The focus is on eight so-called health determinants: Non-smoking, physical activity, diet, body weight, stress management, control of blood pressure, lipid and glucose metabolism.
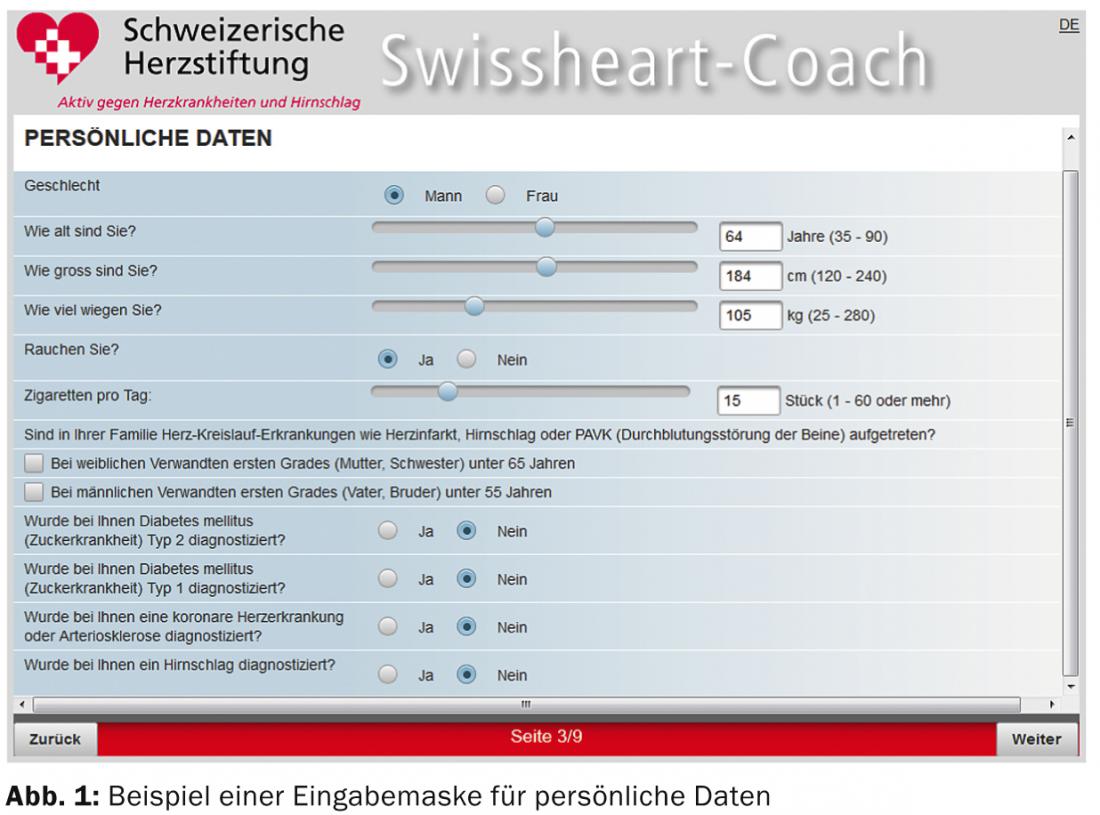
At www.swissheart -coach.ch, it is a risk calculator that primarily represents the relative increase in cardiovascular disease risk compared with a person of the same age without modifiable risk factors or with optimized risk factors. The users of the program enter their data in several submasks (Fig. 1). In the program, a resulting potential of so-called health determinants can be interactively exploited to a variable extent by selecting suggested behavioral changes. No data is stored at this stage, but an individualized, printable report with detailed recommendations is generated at the end of a session. In addition, offers are made for further consultations, including telephone and Internet consultation by physicians of the Heart Foundation. Finally, numerous links to existing information resources and support services and to the ELIPS knowledge database of the University Hospital of Geneva appear. A page specifically designed for professionals provides sources for the scientific calculations.
Risk calculation methodology
The determination of the absolute risk is based on the AGLA score in Swissheart-Coach. Like the ESC score, the AGLA score takes into account, compared with PROCAM, the results of the MONICA study, according to which Switzerland is a low-risk country within Europe, with a weighting factor of 0.7 [1]. Next, the prognostic significance of BMI, number of cigarettes smoked (rather than simply indicating yes or no for smoking), and physical activity is used to calculate relative risk based on the independent significance of these parameters collected in multivariate regression analyses [2–4].
Representation of all included variables
The following variables are used for risk stratification or risk qualification: Age, sex, systolic blood pressure, total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides according to the ESC Prevention Guidelines [5], BMI, number of cigarettes smoked daily, and physical activity calculated as calories burned per week [6, 2] based on metabolic equivalents (MET).
Diet is assessed for its gradual correspondence to the Mediterranean diet according to the alternative Mediterranean score [7]. The stress factor is included in the risk assessment according to the Interheart study [8]. If there are more than three risk factors, an adjusted weighting is applied.
Since it cannot be assumed that all users will be able to provide all the desired data, procedures had to be found for dealing with missing data. If the user does not know his blood pressure and blood lipid data, the system assumes upper non-pathological values and points out the limited informative value of the calculation and requests that the unknown data be determined during a visit to the general practitioner or pharmacy.
Presentation of the results in layman’s terms
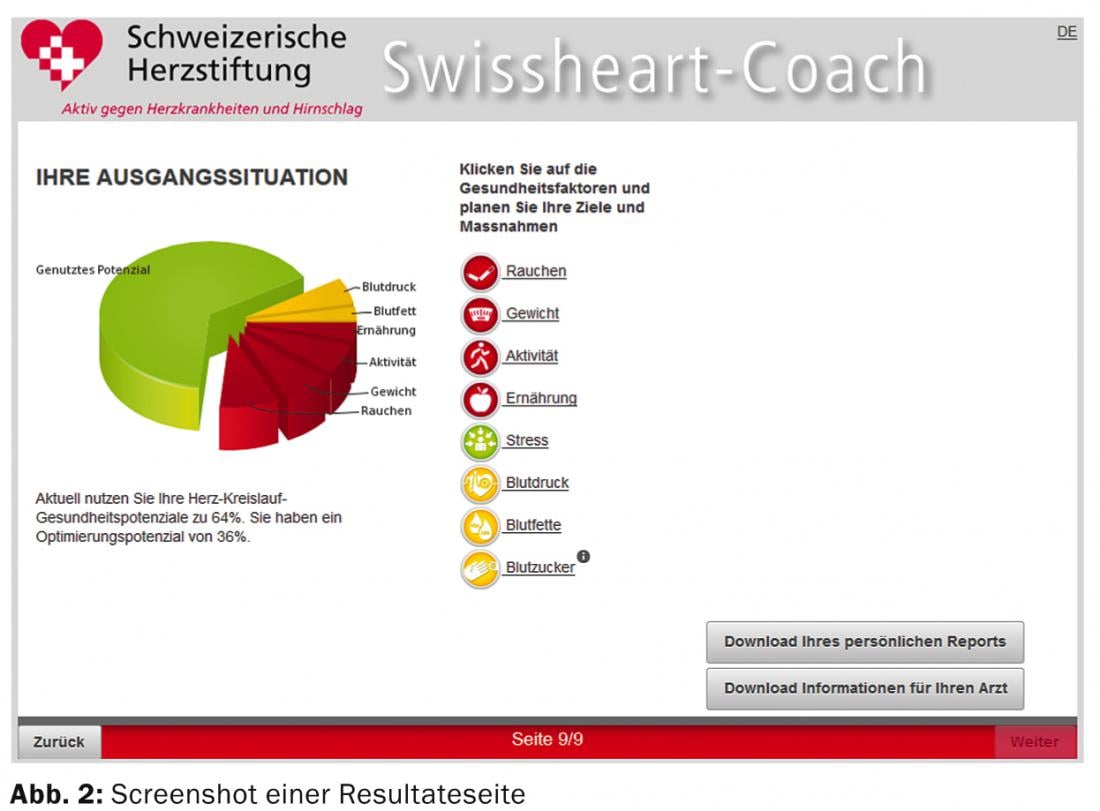
The risk calculators available in the medical community are designed for use by experts. Therefore, in the development of the program, great importance was attached to making it layman-friendly. A categorization of the absolute cardiovascular risk into the levels low, medium, high and very high is performed first. Furthermore, the user learns his calculated heart age. Finally, the relative risk is calculated. This is a comparison of the user to a person with optimal health behavior. The respective expression of the eight health determinants considered for this purpose is quantitatively represented by traffic light colors in a graph (Fig. 2). The interventions and the associated changes are also implemented graphically.
Motivation to mobilize own resources
The particular strength of Swissheart-Coach lies in the fact that this program establishes a dialogue with the user and motivates him to activate his health resources. Users are offered a wide range of possible behaviors to choose from, each of which is acknowledged in a motivating manner. In a second project phase starting in 2014, it should be possible to enter and store individual data at different points in time and to use a user-selectable recall modality for progress monitoring.
In several places, users are informed that further offers exist, and they are provided with Internet links or other contact details. In particular, reference is made repeatedly to primary care physicians, who should be the first point of contact for interpreting and implementing the chosen behavioral changes or for any diagnostic clarifications that may be recommended. Furthermore, the Heart Foundation has been offering a well-established telephone and internet counseling service for some time, which is also referred to and can be further expanded in the future, aligned with the Swissheart Coach. For their part, professionals receive support in the form of in-depth information and pointers to training opportunities.
Discussion and outlook
With the approach described, the Swiss Heart Foundation is breaking new ground in many respects. Methods are used to calculate cardiovascular risk that, although comparable to conventional risk models, were also based in part on similar data. What is new, however, is a greater differentiation of individual variables such as diet and exercise habits, the quantitative consideration of nicotine consumption, and the inclusion of psychosocial factors. The presentation of the calculated risk is primarily as a relative increase compared to a person who optimizes all modifiable parameters and thus has no potential for change. The individually available potential for change is quantitatively represented as a function of the measures selected by the user.
While an individual’s relative risk may be weighted differently from an absolute risk perspective, mobilizing health resources to influence relative risk is important even at low baseline risk when considering the lifetime-risk aspect of these mostly young individuals.
The question of the effect of this offer requires careful scientific monitoring. A cohort study is planned over a defined period of time using a sample of anonymized users in phase II of the project compared to a control collective before the switch-on.
Prof. Dr. med. Andreas Hoffmann
Literature:
- Riesen WF, et al: Schweiz Aerztezeitung 2005; 86: 1355-1361.
- Gohlke H, et al: Eur J Cardiovasc Prev Rehabil 2007; 14: 141-148.
- Gohlke H, et al: Cardiology 2012; 6: 63-76.
- Gohlke H, et al: Cardiology 2012; 6: 249-262.
- Perk J, et al: European Heart Journal 2012; 33: 1635-1701.
- Teo KK, et al. [on behalf of the INTERHEART Study Investigators]: Lancet 2006; 368: 647-658.
- Mitrou PN, et al: Arch Intern Med 2007; 167: 2461-2468.
- Yusuf S, et al. [on behalf of the INTERHEART Study Investigators]: Lancet 2004; 364: 937-952.
CARDIOVASC 2014; 13(1): 14-17









