While vaginal cancer is a rarity, cases of vulvar cancer have increased significantly worldwide over the past 20 years. It is the female carcinoma whose incidence is increasing most rapidly. If precancerous lesions are detected, treated and monitored in time, the prognosis is good. A manifest cancer, on the other hand, often results in serious operations and not infrequently lethal recurrences. Pre- and aftercare are therefore all the more important – also in older patients and after hysterectomy.
Both vulvar and vaginal carcinoma frequently arise in connection with HPV (human papillomavirus) infections (Fig. 1). Differences and similarities were explained by Prof. Andreas Günthert, MD, of the gyn-zentrum Luzern, Switzerland, at the FomF Update Refresher Gynecology, which was held in Zurich, Switzerland, from December 2 to 4 . The conclusion: The impact of both diseases on quality of life is often considerable, not least because of the therapy required, and many cases could be prevented by adequate pre- and post-treatment care. The known precancerous lesions play an important role.
Vaginal carcinoma – a rarity
As a medical rarity, the diagnosis of “vaginal carcinoma” is made less than 50 times a year in Switzerland, with an incidence of 0.4-1.2/100 000 women. It mostly affects older patients, with 15% of cases occurring between the ages of 20 and 49 . It is usually squamous cell carcinoma, arising from precancerous lesions and often HPV-associated. With a 5-year overall survival rate of 54%, the prognosis is rather unfavorable, which, according to Prof. Günthert, may be due in part to the lack of attention to this clinical picture and the often subclinical courses. The often non-specific symptoms such as itching, spotting and dyspareunia also make early diagnosis difficult. The risk factors for developing vaginal carcinoma are similar to those for cervical carcinoma, with promiscuity and smoking at the top of the list. Special attention should be given to patients with status post hysterectomy for invasive or preinvasive lesion, because recurrence of HPV-associated lesions in the vagina may well occur. These are classified as recurrence for the first ten years after hysterectomy and as neoplasia of vaginal origin thereafter.

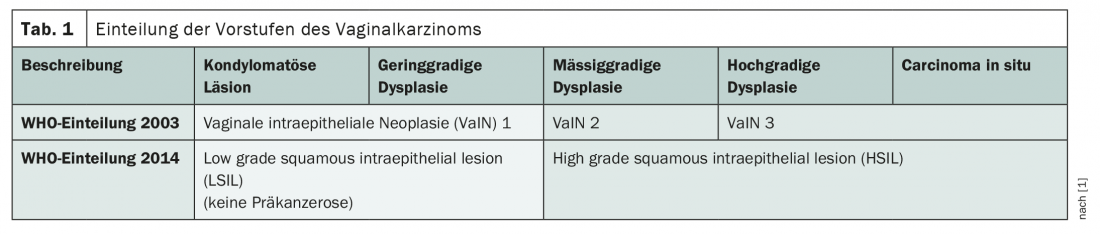
Classically, vaginal carcinoma develops from vaginal intraepithelial neoplasia (VaIN), with only two categories according to the current WHO classification: Low-grade Squamous Intraepithelial Lesion (LSIL) and High-grade Squamous Intraepithelial Lesion (HSIL) (Tab. 1). LSIL, which corresponds to the former VaIN 1, is no longer considered a precancerous condition, which is intended to prevent overtreatment. The data situation regarding lichen sclerosus and lichen planus as potential precancerous lesions is more unclear. Here, there is a lack of meaningful studies to assess their risk of degeneration. The conversion rate of HSIL to carcinoma is approximately 2-5% – and adequate therapy can prevent progression. This usually consists of laser treatment, with more than half of precancerous lesions recurring. So good aftercare is of great importance. As an alternative to laser therapy, imiquimod can be used off-label. Here, the cure rate is about 86% – but often with significant side effects. Brachytherapy is also used in extensive cases, but this requires long-term care of the vaginal skin to prevent adhesion. Apart from therapy and follow-up, prevention of precancerous lesions is also important to prevent the development of vaginal carcinoma. Thus, HPV vaccination brings an estimated risk reduction of about 60%. Regular PAP and HPV testing, especially after hysterectomy for cervical cancer or a preinvasive lesion, can also help detect any precancerous lesions and recurrences as early as possible.
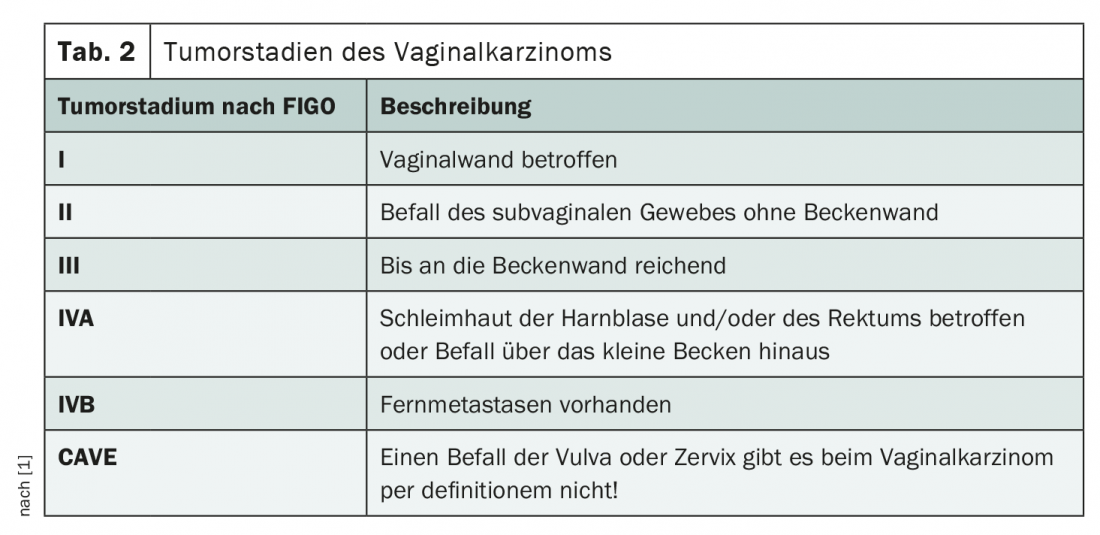
If vaginal carcinoma occurs, it is classified according to the FIGO classification (Table 2) . It should be noted that, by definition, there must be no involvement of the vulva or cervix. This is because even if most of the tumor burden is in the vagina, but vulva or cervix are affected, the malignancy is considered either cervical or vulvar carcinoma. The therapy of vaginal carcinoma is difficult due to its rarity and the sparsely populated study landscape. Most therapeutic considerations arise by analogy with recommendations in cervical and vulvar cancer. In principle, interdisciplinary management is required. While surgery via colpectomy or hemicolpectomy and, if necessary, hysterectomy is the primary approach for localized tumors (FIGO I), surgery must be weighed against primary radiochemotherapy for stage II-IV carcinomas. It should be noted here that irradiation of the pelvic organs and vaginal skin is problematic, especially in sexually active women. According to Prof. Günthert, the operation may well be beneficial in terms of quality of life. However, a good reconstruction is indispensable and often complex to perform. For stage I tumors with a maximum diameter of 4 cm and negative lymph node findings on imaging, sentinel lymph node biopsy (SLNB) is increasingly performed starting at an infiltration depth of 1 mm. This is sometimes difficult given the complex and variable lymphatic drainage pathways. It must be remembered that the upper vaginal third tends to drain pelvically, the lower third tends to drain inguinally, and the middle third drains in both directions. Thus, pelvic and inguinal detection is targeted. Depending on the findings, this may entail lymph node dissection, debulking and, if necessary, post-radiation.
The vulva: a complex organ
In contrast to vaginal carcinoma, the data for vulvar carcinoma is more solid. As a less hormone-dependent and anatomically far more complex organ, the vulva is significantly more susceptible to cancer. In his lecture, Prof. Günthert addressed the importance of anatomy for the diagnosis and treatment of vulvar cancer, in particular the different compartments. In the anatomical classification, ontogenetic origin plays an important role. Thus, the vulva in the strict sense develops separately from the labia majora, mons pubis and anus. Only the ventral anus portion between 11 and 1 o’clock strictly belongs to the gynecology and middle subcompartment of the vulva. Thus, a carcinoma in this area would be a vulvar carcinoma and not an anal carcinoma. According to Höckel et al. the ontogenetic vulva can be divided into three compartments: The inner vulva, which includes the vestibule, the middle vulva with glans and labia minora, and the outer vulva, the interlabial space.
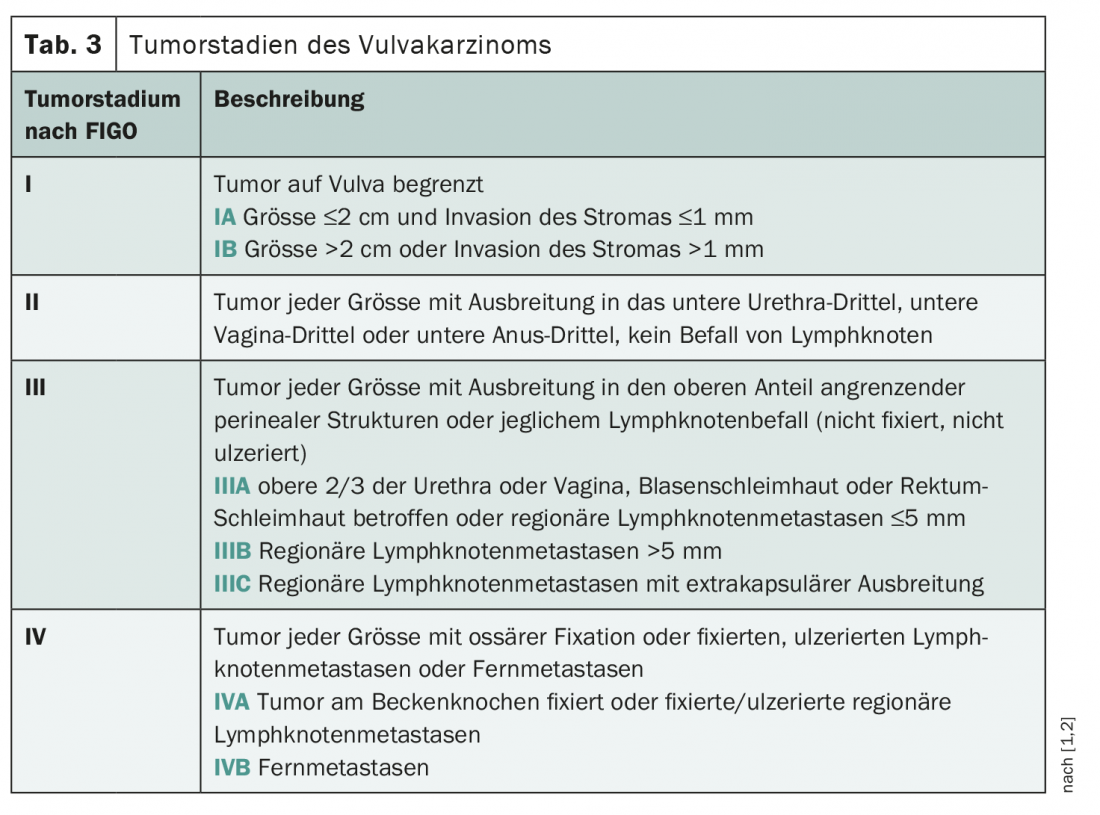
The staging of vulvar carcinoma was adapted this year and is based for the first time on prospective data to assess prognosis (Table 3) [2]. While this tends to be favorable in HPV-positive carcinomas, it is less favorable in HPV-negative cases and very poor in inguinal or pelvic lymph node recurrence. Thus, good follow-up care is also of utmost importance in vulvar cancer. Here, inguinal recurrences can be detected early by ultrasound, for example. Overall, more than three-quarters of recurrences occur in the first three years. Local recurrence affects 20-50% of patients, of whom 70% experience at least a second recurrence. In contrast, groin and pelvic recurrences occur in 3-9% of cases-with a historical 5-year overall survival rate of less than 25%. However, this has been significantly improved over the last few years by SLNB and appropriate management by surgery, radiation, and chemotherapy when appropriate. For example, in a more recent analysis, half of women with inguinal recurrence of vulvar cancer were still alive after six years [3]. Risk factors for disease return include lymph node metastases, lichen sclerosus, and resection not in a healthy setting.
The therapy of vulvar carcinoma is a great challenge for physicians and patients, not only because of the high recurrence rate. The high complication rate and long-term damage of the therapy are also problematic. Thus, wound healing disorders and lymphedema often occur after lymphadenectomy. To prevent wound healing problems, Prof. Günthert recommends a prophylactic relief stoma of the bowel for three months after surgery, but this is often met with resistance by patients. Reconstructive technique by means of flapplasty has a great importance for the quality of life. For example, only a good reconstruction allows tension-free sitting, not to mention sexual intercourse. This requires a high level of expertise among physicians and also in nursing, which can be ensured by specialized Pelvic Care Nurses , among others. The surgical approach to vulvar cancer is undergoing constant change, with a current focus on safety margin and lymph node management. Whereas 8 mm safety distance was recommended in the past, today it is 5. However, according to Prof. Günthert, 2 mm is probably sufficient. And things are also happening at the SLNB. Thus, double labeling using technetium and patent blue could soon be replaced by technetium and indocyanide green (ICG). A recent study also showed that combined inguinofemoral lymphadenectomy with radiotherapy was superior to radiotherapy alone when lymph node involvement exceeded 2 mm [4].
Regarding the systemic therapy of vulvar carcinoma, many questions currently remain unanswered. Thus, adjuvant therapy has never been systematically studied, and recommendations are mostly extrapolations from cervical cancer studies. Currently, systemic therapy consists of a multimodal approach with chemoradiotherapy. However, checkpoint inhibitors may also be increasingly used in vulvar cancer in the near future, for which only isolated case reports exist to date. Electrochemotherapy – a procedure particularly suitable for superficial malignancies – could also become more important. The ELECHTRA study is currently underway for this purpose.
Overview of precancerous lesions of the vulva
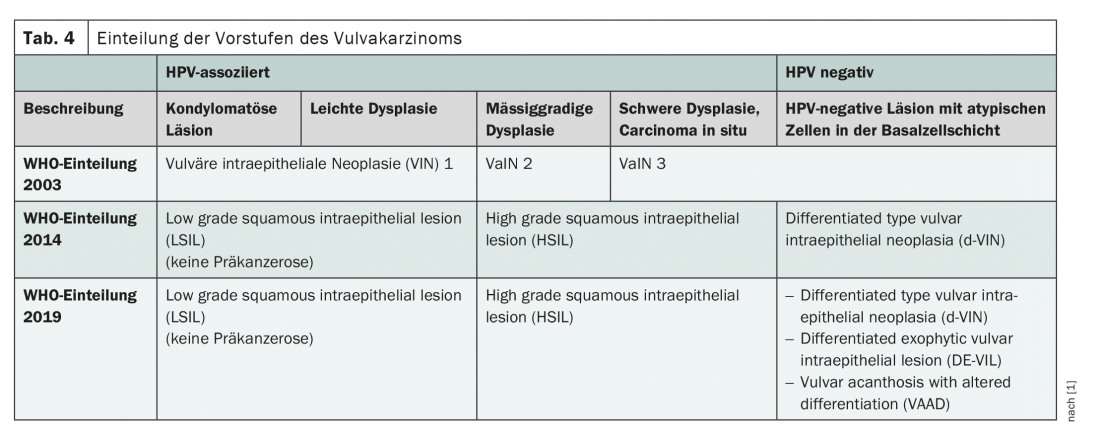
As with vaginal carcinoma, precancerous lesions also play a significant role in the development and thus prevention of vulvar carcinoma. Their incidence has increased by 400% in the last 20 years, leading to a parallel increase in carcinoma cases. The classification of precancerous lesions was adapted two years ago (Tab. 4) . In principle, a distinction is made between HPV- and non-HPV-associated lesions, and there are now three categories of non-HPV-associated precancerous lesions. However, these do not include all precancerous lesions, as Prof. Günthert pointed out. For example, Paget’s disease is still not represented in the classification. Currently, there are three known pathways by which precancerous lesions of the vulva develop into carcinomas. The highest rate of degeneration is found in non-HPV-associated precancerous lesions with a p53 mutation. These develop into vulvar carcinoma in over 80% of cases. Another pathway of carcinogenesis of non-HPV-associated precancerous lesions is via alternative mutations such as PIK3CA, HRAS, or PTEN. Overall, these two pathogenetic pathways account for 40-50% of vulvar cancers and are more likely to affect older patients. The remaining 50-60% of vulvar carcinomas arise from HPV-associated precancerous lesions. HSILs are very commonly diagnosed, but develop into carcinoma in only 4-9% of cases. It is important to note that once high-risk HPV infection is detected at the cervix, the risk for vulvar precancerous lesions is also higher. For example, an unpublished study from the Lucerne Women’s Hospital showed that 83% of patients who underwent HPV-related conization were also HPV-positive in the vulva. The consequence: After conization, the expert recommends regular follow-up examinations, which should include the vulva.
If HSIL of the vulva is detected, therapy is usually by laser treatment or surgery – with a recurrence rate of 51%. So follow-up is extremely important here as well. Analogous to HSIL of the vagina, off-label imiquimod can also be used. Cidofovir is being studied in this indication. According to the current data, HPV vaccination is able to reduce the local recurrence rate after HSIL. Due to the higher risk of degeneration, a dVIN (differentiated type Vulvar Intraepithelial Neoplasia) must be resected in healthy tissue. Lichen sclerosus, as a precursor of d-VIN, also requires good therapy and annual vulvoscopies to prevent carcinoma development. This occurs in about 3-7% of cases and has been shown to be lower with good compliance.
Congress: FomF Update Refresher Gynecology
Source:
- Lecture “Update gynecologic oncology: vulva and vagina” by Prof. Dr. med. Andreas Günthert at the Forum for Continuing Medical Education (FomF) Update Refreshers Gynecology, 03.12.2021, Zurich.
Literature:
2 Olawaiye AB, et al: FIGO staging for carcinoma of the vulva: 2021 revision. Int J Gynaecol Obstet 2021; 155(1): 43-47.
3 Frey JN, et al: Should Groin Recurrence Still Be Considered as a Palliative Situation in Vulvar Cancer Patients? A Brief Report. Int J Gynecol Cancer 2016; 26(3): 575-579.
4. Oonk MHM, et al: Radiotherapy Versus Inguinofemoral Lymphadenectomy as Treatment for Vulvar Cancer Patients With Micrometastases in the Sentinel Node: Results of GROINSS-V II. J Clin Oncol 2021; 39(32): 3623-3632.
InFo ONCOLOGY & HEMATOLOGY 2022; 10(2): 20-22.