
At the 29th Swiss Annual Conference on Phytotherapy in Winterthur, the question was posed as to what possibilities phytotherapeutic approaches offer in the therapy of benign prostate syndrome, prostatitis or pelvic pain syndrome, and prostate carcinoma. An overview of the study situation in recent years was provided by Matthias Rostock, MD, Hamburg/Zurich.
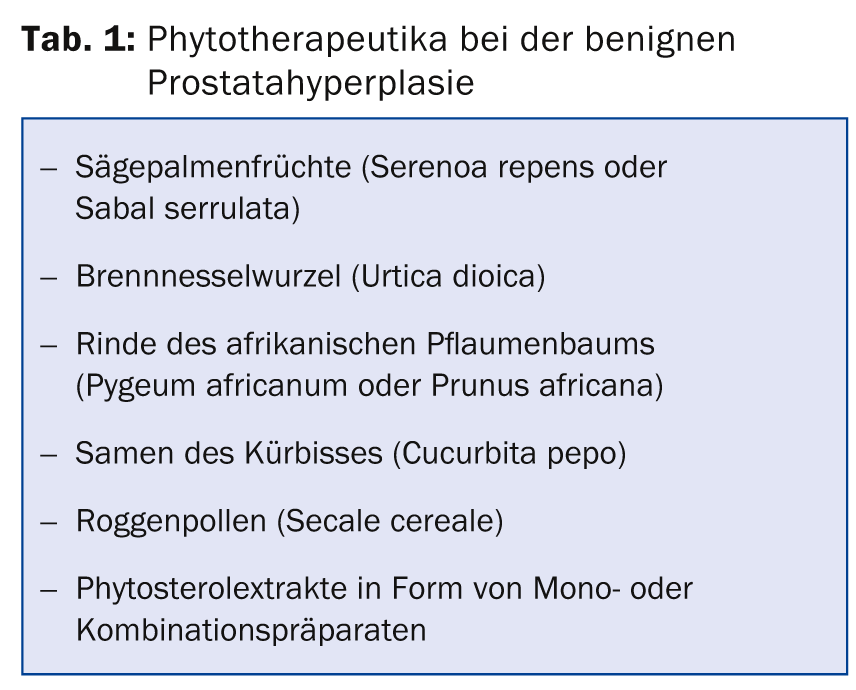
(ag) The term “benign prostatic syndrome” is now used for benign prostatic enlargement that occurs together with lower urinary tract symptoms (weakened urinary stream, delayed urination, dribbling, residual urinary sensation). In addition, pollakisuria, nocturia, alguria, and repeated imperative urination (with increasing symptoms of urge incontinence) are common. In the guidelines on drug therapy, the successes of phytotherapeutics are usually considered to be difficult to assess, since the evidence from studies obtained to date does not yet allow a firm conclusion to be drawn in its entirety. “Nevertheless, there is a great demand on the part of patients for such phytotherapeutic treatments – not least because synthetic preparations cause more side effects such as fatigue, dizziness, headache, diarrhea, and drop in blood pressure (α-1-receptor antagonists), loss of libido, erectile dysfunction and swelling of the mammary gland (5-α-reductase inhibitors), as well as confusion, memory and sleep disturbances and an increased risk of acute urinary retention (muscarinic receptor antagonists),” explained Dr. Matthias Rostock, MD, Hamburg/Zurich. An overview of possible phytotherapeutic agents in this area is given by Table 1. Numerous controlled therapy studies have shown an association with improved subjective symptoms in benign prostatic hyperplasia, but in view of the increased demands on research methodology (on the part of the international WHO-BPH consensus conferences), some recent studies have not been able to confirm the results of earlier research.
Prostatitis and CPPS
Prostatitis that is acutely bacterial in nature and accompanied by fever and a severe feeling of illness requires immediate, targeted, and high-dose antibiotic treatment. The same is true for chronic bacterial prostatitis. However, an accurate differential diagnosis to chronic abacterial prostatitis (congestive prostatitis) and chronic non-inflammatory pelvic pain syndrome (CPPS) should be performed first (both belong to NIH classification III). The latter is a complex psychosomatic clinical picture that can be accompanied by non-specific, sometimes radiating pain symptoms in the perineal area as well as complaints of the lower urinary tract (increased urge to urinate, difficult and painful urination with dribbling and residual urine sensation). Loss of libido, erectile dysfunction and pain during intercourse may also occur. In addition to established treatment approaches such as psychotherapy, relaxation exercises, and nutritional concepts, there are positive phytotherapeutic studies on a rye pollen extract and a preparation containing quercetin [1,2].
Prostate Cancer
In prostate cancer, phytotherapy can be helpful at various stages as an adjunctive or stand-alone measure.
High-grade prostatic intraepithelial neoplasia (HGPIN): this premalignant prostatic change is often discovered by a prostate biopsy ordered because of an elevated PSA level. The risk of developing invasive prostate cancer is significantly increased with this diagnosis, but there is no established strategy for prevention. An Italian prospective randomized double-blind study [3] with 60 patients compared the therapeutic effect of a green tea extract with that of placebo. Study participants took one capsule containing 200 mg of green tea extract three times daily. Over the course of one year, nine new cases of invasive prostate cancer were diagnosed in the placebo group (n=30) by control biopsy. In the verum group (n=30), this was true for only one patient. Thus, there was a statistically significant difference, which was confirmed at follow-up (two years later). A larger subsequent Phase III study is currently underway.
PSA recurrence after curatively intended primary therapy: A renewed increase in the PSA value after primary treatment of invasive prostate carcinoma indicates a recurrence. An uncontrolled phase II study [4] examined the effect of 240 ml of pomegranate juice containing 570 mg of polyphenols taken daily in 46 men (after surgery or radiation therapy had been performed). The PSA doubling time, a classic way to monitor progression, could thus be significantly extended from an average of 15 (before treatment or baseline) to 54 months (under treatment). Tolerance was good. A subsequent randomized trial [5] in which 104 patients with rising PSA levels after previous curative intentional primary therapy received 1 or 3 g of pomegranate extract (1000 or 3000 mg polyphenol content, respectively) also showed a significant increase in PSA doubling time compared with baseline. The different dosage did not play a statistically significant role. Of course, according to Dr. Rostock, the initially quite promising results need to be confirmed in further controlled studies. Furthermore, it should not be forgotten that in the case of a slow-rising PSA, radiotherapeutic treatment can be secondarily curative, which clearly limits the use of complementary therapeutic measures.
Recently, results of a placebo-controlled study [6] with 199 participants (PSA recurrence, completed primary treatment) on the combination preparation of pomegranate, green tea, broccoli and curcuma extract were presented – significant delays of the PSA increase were also found. In addition, the verum group showed significantly more cases of PSA decline or stabilization (46%) than placebo (14%). Side effects were registered in 34% in the placebo group and in 24% in the verum group (not significant). Gastrointestinal complaints, however, occurred more frequently here. One man suffered from grade 2 diarrhea while on verum. Side effects of grade 3 or higher did not occur.
Source: “The Potential of Phytotherapy in Diseases of the Prostate with a Focus on Prostate Carcinoma”, presentation at the 29th Swiss Annual Conference on Phytotherapy,
18-21 June 2014, Winterthur
Literature:
- Wagenlehner FM, et al: A pollen extract (Cernilton) in patients with inflammatory chronic prostatitis-chronic pelvic pain syndrome: a multicentre, randomised, prospective, double-blind, placebo-controlled phase 3 study. Eur Urol 2009 Sep; 56(3): 544-551.
- Shoskes DA, et al: Quercetin in men with category III chronic prostatitis: a preliminary prospective, double-blind, placebo-controlled trial. Urology 1999 Dec; 54(6): 960-963.
- Bettuzzi S, et al: Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study. Cancer Res 2006 Jan 15; 66(2): 1234-1240.
- Pantuck AJ, et al: Phase II study of pomegranate juice for men with rising prostate-specific antigen following surgery or radiation for prostate cancer. Clin Cancer Res 2006 Jul 1; 12(13): 4018-4026.
- Paller CJ, et al: A randomized phase II study of pomegranate extract for men with rising PSA following initial therapy for localized prostate cancer. Prostate Cancer Prostatic Dis 2013 Mar; 16(1): 50-55.
- Thomas R, et al: A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer-the UK NCRN Pomi-T study. Prostate Cancer and Prostatic Disease 2014; 17: 180-186.
HAUSARZT PRAXIS 2014; 9(9): 37-38









