
After a stroke, driving ability may be impaired. Patients must therefore have their physical and mental fitness checked by specialists. A comprehensive assessment in the sense of a 4-step model is useful: neurological examination, neuropsychological and traffic psychological testing procedures, and driving with a driving simulator or, where indicated, with a clinic driving instructor. If the 4-step plan does not bring a clear decision, the control drive at the road traffic office may be necessary. This is done with an expert from the road traffic office and possibly a traffic physician or traffic psychologist. Driving fitness assessments by primary care physicians in collaboration with a driving instructor are not purposeful because the driving instructor cannot assume the role of an expert.
After a stroke, driving ability may be impaired due to motor or neuropsychological limitations. To determine fitness to drive, it is necessary to verify physical and mental fitness.
The Swiss Traffic Licensing Ordinance (VZV) stipulates: Anyone with a serious illness must have their fitness to drive determined by a specialist. If he does not provide this proof and has an accident, the vehicle insurance and/or the liability insurance will not cover any damage (even if he is not the causer).
In Switzerland there are freelance traffic psychologists FSP/VfV or working at an institute for forensic medicine, who are listed in the VZV and are commissioned to clarify character and performance aspects of suitability. By law, the traffic psychologist is authorized to assess cognitive performance parameters important to fitness to drive, as well as issues related to character aptitude (emotional stability and behavior). It is increasingly common for neuropsychologists at hospitals, without specific training, to comment on fitness to drive. In any case, this seems to be problematic if the neuropsychologist does not have postgraduate training (SVNP, Swiss Association of Neuropsychologists, and FSP, Federation of Swiss Psychologists). Driving suitability assessments by general practitioners in collaboration with a driving instructor are not to be considered purposeful, since the driving instructor cannot assume the role of an expert. For example, he does not know how neglect or frontal brain syndrome affects driving. Practical driving tests must be carried out by the road traffic office of the canton of residence (possibly together with a traffic physician or traffic psychologist) or by another authorized institution.
Performance and character
After a neurological event, a comprehensive assessment, as provided by the 4-stage model in the Valens Clinics, is useful:
- Neurological examination
- Neuro- and traffic psychological test procedures
- Rides with a driving simulator SMART
- Ride with clinic driving instructor where indicated.
In the case of neurological events such as stroke, the specialist must survey neurological aspects (motor impairment, epilepsy, visual field and medication) and assess them with regard to fitness to drive. Then, after registration by the neurologist, the patient must complete a neuro/traffic psychology test examination. The following performance domains are examined: directed and divided attention, cognitive flexibility, psychomotor speed, impulse control, visuospatial and peripheral perception, processing speed, spatial orientation, and tracking.
A study [1] has shown that patients with mild to sometimes moderate performance deficits can demonstrate compensatory strategies in the SMART driving simulator (Fig. 1) that allow them to still pass the driving test.
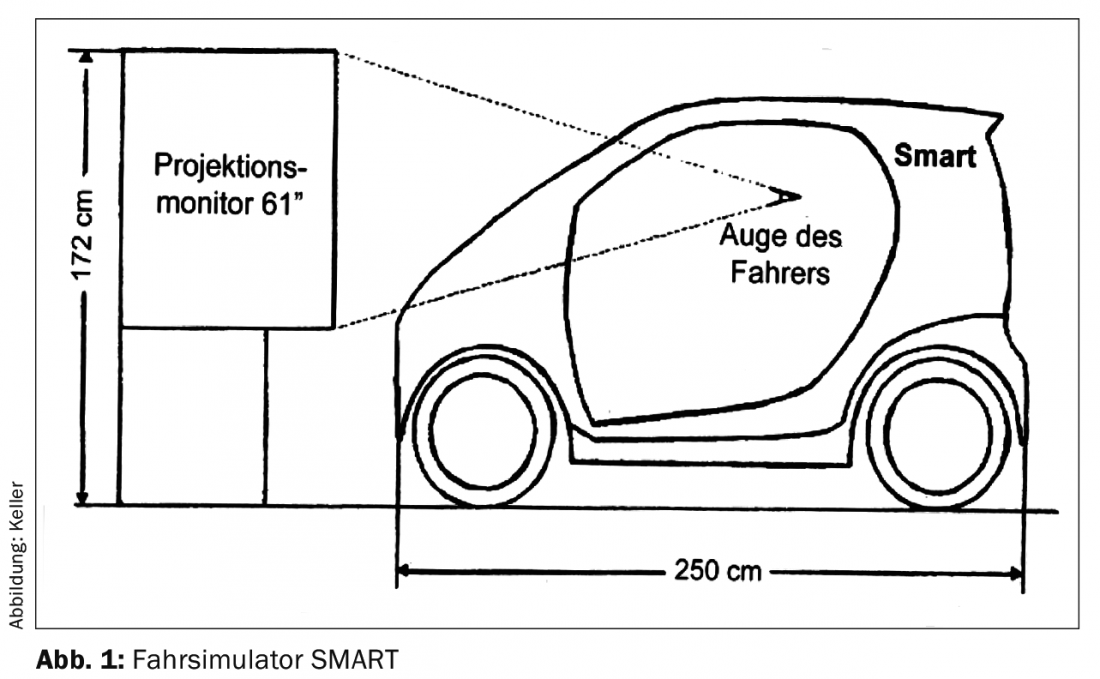
In principle, patients must complete two journeys in the SMART driving simulator, whereby the second journey must not show any gross errors (accident, difficulties in keeping in lane). The driving simulation option is also used when it is unclear how a person will react in their emotional behavior to a complex drive.
If driving with the driving simulator still presents uncertainties, a ride with the clinic driving instructor can be arranged. The Road Traffic Offices of the cantons of St. Gallen and Graubünden have appointed a driving instructor to carry out a standardized route of one hour (mountain route, freeway, interurban, city driving). Neuropsychological and traffic psychological test diagnostics alone have only limited informative value regarding fitness to drive [2,3].
Recover driving performance on the simulator
Various publications have shown, in the case of a negatively assessed fitness to drive, that predictors of performance on the driving simulator (Fig. 2) are positively related to the actual, practical driving test [4–6].

The driving simulator in neurological rehabilitation leads to marked learning gains in patients after only six training drives in terms of variable lane keeping, visual exploration, divided attention, and choice of driving speed [4]. Brain-injured people after stroke can benefit from such driving training.
Fitness to drive
Finally, some questions relevant to practice will be answered.
- Which clarification should take place when? As described above, a step-by-step approach can be taken. From a medical point of view, the specialist in neurology must generally affirm fitness to drive. Satisfactory performance on psychological testing procedures constructed for fitness to drive may be sufficient (if no emotional behavioral problems are evident). If neuropsychological/traffic psychological performance impairments are found, two drives on the SMART driving simulator can provide the decisive result for assessing fitness to drive. If the result in the driving simulator is faltering, it may be useful to arrange a ride with the clinic driving instructor.
- When is a check at the road traffic office necessary? If the 4-step plan does not allow a clear decision, the control drive at the road traffic office may be necessary. If a patient is unresponsive and it is suspected that he or she will not comply with the driving ban in connection with the brain-organic impairment, the physician must report the patient to the road traffic office. If an adaptation of the vehicle is necessary (e.g. in the case of severe hemiplegia), it is also essential to consult the Road Traffic Office.
- Should the primary care physician work with the driving instructor to determine fitness to drive? A brain injury can manifest itself in various ways while driving (neglect, hemianopsia, frontal brain syndrome, emotional instability, anosognosia, etc.), which is why an expert from the road traffic office must conduct the check ride with a traffic physician or traffic psychologist.
Literature:
- Keller M, et al: On compensation strategies in the driving simulator for driving fitness. In: Schubert W, Mattern R, Nickel WR (eds.): Test methods of driving fitness assessment in psychology, medicine and engineering. Schriftreihe Fahreignung. Bonn, Kirschbaum Verlag 2008; 108-110.
- Dettmers C, Weiller C: Fitness to drive in neurological disorders. Bad Honnef, Hippocampus 2004.
- Niemann H, Hartje W: Assessment of driving fitness of brain-injured patients in neurological rehabilitation. Zeitschr f Neuropsychologie 2013; 24(2): 69-87.
- Keller M, et al: Driving simulator in neurological rehabilitation. Neurol Rehabil 2004; 10(3): 137-143.
- Casutt G, et al: The relation between performance in on-road driving, cognitive screening and driving simulator in older healthy drivers. Transportation Research Part F 2014; 22: 232-244.
- Casutt G, et al: The drive-wise project: driving simulator training increases real driving performance in healthy older drivers. Frontiers in Aging Neuroscience 2014; 6: 85.
InFo NEUROLOGY & PSYCHIATRY 2015; 13(6): 14-17.









