
As shown by large skin cancer registries and population-based studies, there is a continuing trend in Europe and worldwide towards an increase in new cases of melanocytic and non-melanocytic tumors. In particular, squamous cell carcinomas (cSCC) and basal cell carcinomas (cBCC) are predicted to have a high increase in incidence. Because most metastases in squamous cell carcinoma occur within two to three years after diagnosis of the primary tumor, this phase is an important window of opportunity for secondary prevention.
Valid registry data provide an important basis for reliable epidemiologic analyses [1]. The largest population-based skin cancer registries include the Global Cancer Observatory, the European Cancer Information System (ECIS), and the International Agency for Research. According to the Global Cancer Observatory (IARC), there are approximately 300 000 new cases of melanoma worldwide, with approximately half occurring in Europe [2]. In Switzerland, melanocytic tumors are the fifth most common type of cancer, with approximately 2800 individuals diagnosed annually, with almost a quarter of those diagnosed being under 50 at the time of initial diagnosis [3]. Early detection and treatment have improved significantly in recent years, although there are certain differences within Europe in this regard, explains Prof. Ana-Maria Forsea, MD, of Elias University Hospital and Carol Davila University of Medicine and Pharmacy, Bucharest (Romania). Data from the ECIS registry on melanoma show that in Central Europe, the 5-year survival rate is significantly higher compared with Eastern European countries, indicating disparities in care, the speaker said [1,4].
Trend toward increase in skin cancer incidence continues
In Switzerland, as well as in Europe as a whole, there is a trend towards an increase in the incidence of melanoma, although survival rates are relatively good compared to other tumor types. Thus, according to the Federal Office of Public Health (FOPH), the 5-year survival rate in Switzerland is over 80% [5]. However, as age-stratified analyses of a large population-based study over the 30-year period show, mortality trends vary with age and other factors [6].
The incidence of non-melanocytic tumors (NMSC) has also increased in recent years. The greatest risk factors are known to be UV radiation exposure and advanced age. White skin cancer accounts for over 90% of all skin cancer cases, with approximately 20-30% being squamous cell carcinoma (cSCC) and 70-80% being basal cell carcinoma (cBCC) [1]. Because NMSC is not included in most large skin cancer registries, epidemiologic data on it are based on other data sources such as studies or smaller local registries. According to experts, a marked increase in new cases is expected in Europe in the coming years; it is estimated that in Germany, for example, the incidence of NMSC will double by 2030 [7]. Mortality rates are low, but white skin cancer is associated with significant morbidity.
Metastasis risk: monitoring and patient education
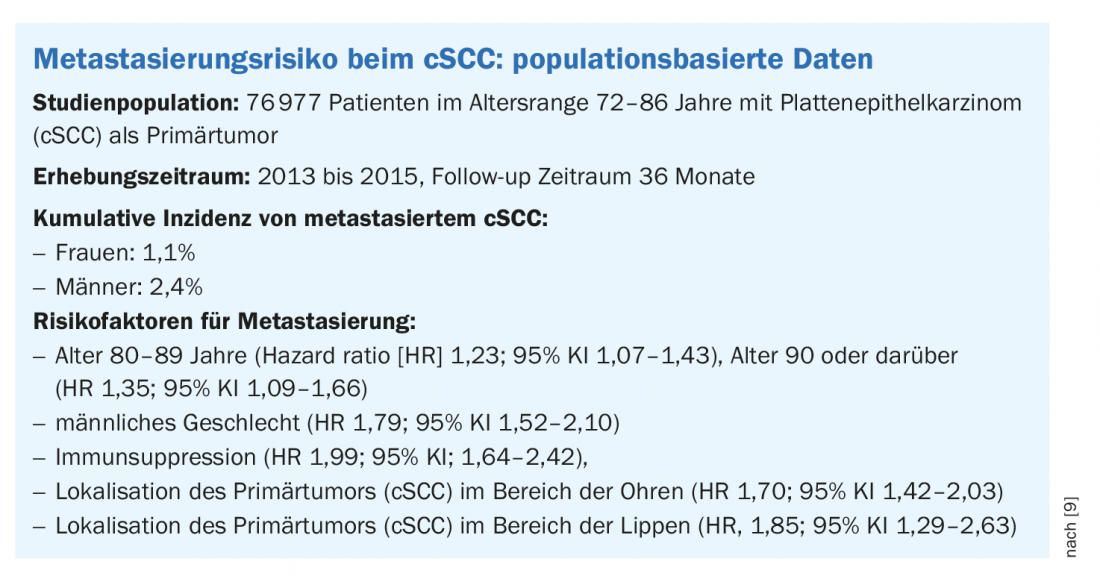
The overall risk of metastasis is estimated to be approximately 4% for squamous cell carcinoma (cSCC) [1]. However, the data in this regard vary depending on the study population and design. Analyses of data collected from 2013 to 2015 from a large population-based study in England (n=76,977, age range 72-86 years) found that 92.9% of metastases occurred within three years of diagnosis of the primary tumor. Age, male sex, immunosuppression, and localization of the primary tumor to the ears and lips were found to be associated with an increased risk of metastasis (Box) [9].
In analyses of an epidemiologic study with a smaller sample (n=1122) in which data were collected from 2005 to 2014, the incidence of metastasis was reported to be 1.2-2%–2,7%, with more than 80% of metastases occurring within two years of diagnosis of the primary tumor [10]. According to the authors, patient education is an important aspect of monitoring during this critical period. Thus, patients should be trained to regularly check for signs of recurrence or possible metastasis and, if necessary, have dermatological clarification performed.
Source: EADV Annual Meeting 2020
Literature:
- Forsea AM: Overview of epidemiology of skin cancer, Prof. Ana-Maria Forsea, MD, EADV Annual Meeting, 10/31/2020.
- International Agency for Research on Cancer (IARC), www.iarc.who.int
- Swiss Cancer League, www.krebsliga.ch/ueber-krebs/krebsarten/hautkrebs-melanom-schwarzer-hautkrebs/
- European Cancer Information System (ECIS), https://ecis.jrc.ec.europa.eu
- Federal Office of Public Health (FOPH), www.bag.admin.ch/bag/de/home/zahlen-und-statistiken/zahlen-fakten-nichtuebertragbare-krankheiten/krebserkrankungen-schweiz.html
- Yang DD, et al: Trends in malignant melanoma mortality in 31 countries from 1985 to 2015. BJD 2020; 183(6): 1056-1064.
- Leiter U, et al: Incidence, Mortality, and Trends of Nonmelanoma Skin Cancer in Germany J Invest Dermatol 2017; 137(9): 1860-1867.
- Laughter MR, et al: The Burden of Skin and Subcutaneous Diseases in the United States From 1990 to 2017. JAMA Dermatol 2020; 1; 156(8): 874-881.
- Venables ZC, et al: Nationwide incidence of metastatic cutaneous squamous cell carcinoma in England. JAMA Dermatol 2019; 155(3): 298-306.
- Nelson TG, Ashton, RE: Low incidence of metastasis and recurrence from cutaneous squamous cell carcinoma found in a UK population: Do we need to adjust our thinking on this rare but potentially fatal event? J Surg Oncol 2017; 116(6): 783-788.
DERMATOLOGIE PRAXIS 2021; 31(1): 46 (published 2/23/21, ahead of print).









