
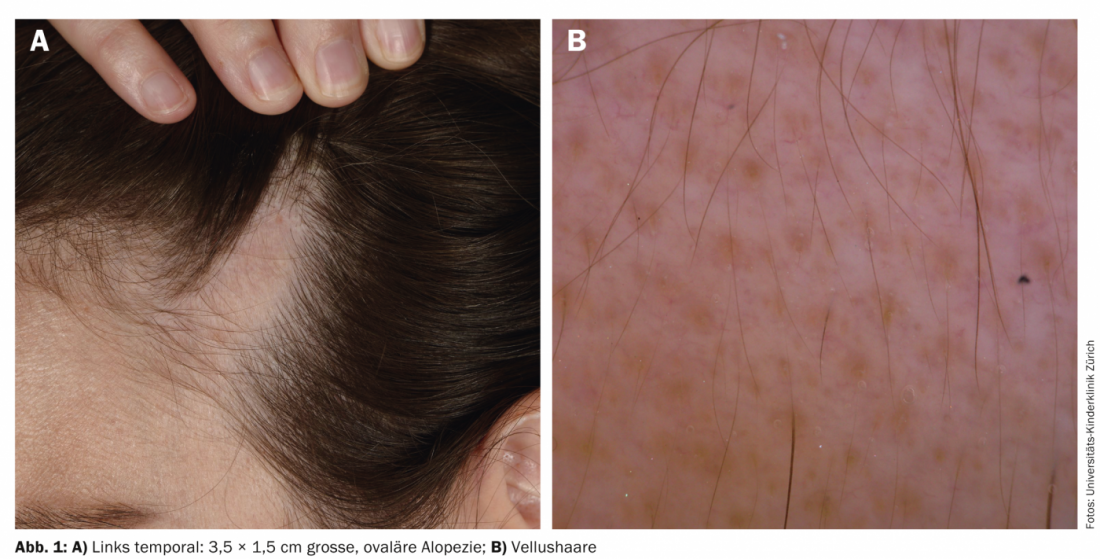
Case report: At the age of two years the parents of the now ten-year-old girl noticed for the first time a hairless area temporally on the left side. At the beginning, this bald spot increased slightly, but then grew proportionally as it progressed. At no time was there itching, flaking or redness of the scalp. The girl is otherwise healthy, but now feels increasingly disturbed by the hairless area. Examination revealed a 3.5 × 1.5 cm oval alopecia temporally on the left side (Fig. 1a). Dermoscopy revealed inconspicuous hair follicle openings with numerous vellus hairs (Fig. 1b). The alopecic area is surrounded by normal terminal hair.
Quiz:
Based on this information, which diagnosis is the most likely?
A Alopecia areata
B Linear morphea (“en coup de sabre”)
C Alopecia triangularis congenita
D Trichotillomania
Diagnosis and discussion: The patient shows the typical findings of alopecia triangularis congenita (ATC, “temporal triangular alopecia”). The first manifestation in infancy, the characteristic localization laterally of the receding hairline with a suggested triangular shape without evidence of atrophy or epidermal involvement are indicative. ATC is rare but likely underdiagnosed and, although congenitally inherited, is often not noticed until the infantile downy hair transforms to terminal hair between the ages of two and four years [1]. The diagnosis can be confirmed dermatoscopically and differentiated from the above-mentioned differential diagnoses. ATC is characterized by preserved follicles with exclusively vellus hairs [2]. Signs of scarring, as found in aplasia cutis congenita or morphea, are absent. Likewise, there is no evidence of exclamation mark or cadaver hair as in alopecia areata or broken hairs as in trichotillomania or traction alopecia, respectively.
As in our patient, usually unilateral, rarely bilateral, an oval, triangular or lancet-shaped circumscribed focus of alopecia appears on the temporal scalp, which grows proportionally with the child and persists throughout life [3]. Occasionally, a central tuft of hair is found (“central 
ATC was first described by Sabouraud in 1905 [5]. The etiology remains unknown; a cutaneous mosaic with abnormal epithelial-mesenchymal interaction is suspected [3]. With few exceptions, ATC occurs sporadically. Girls and boys are affected with equal frequency [1].
In children with congenital local alopecia with a short skull (brachycephaly) and possibly accompanying neurological abnormalities (cerebellar dysfunction, trigeminal anesthesia with absent corneal reflex, developmental disorders), the rare differential diagnosis of Gomez-Lopez-Hernandez syndrome (cerebello-trigeminal dermal dysplasia with rhombencephalosynapsis) should also be considered [6].
If treatment is desired, plastic surgery with excision or hair transplantation may be considered therapeutically for ATC.
Knowledge of this characteristic form of localized alopecia is instrumental in reassuring affected patients and their families and avoiding unnecessary therapies.
Alexandra Smith
Martin Theiler, MD
Regula Wälchli, MD
Lisa Weibel, MD
Literature:
- Lacarrubba F, Micali G: Congenital triangular alopecia. BMJ case reports 2014; 2014.
- Inui S, Nakajima T, Itami S: Temporal triangular alopecia: trichoscopic diagnosis. The Journal of Dermatology 2012; 39: 572-574.
- Yamazaki M, Irisawa R, Tsuboi R: Temporal triangular alopecia and a review of 52 past cases. The Journal of Dermatology 2010; 37: 360-362.
- Assouly P, Happle R: A hairy paradox: congenital triangular alopecia with a central hair tuft. Dermatology 2010; 221: 107-109.
- Sabouraud R: Manuel Élémentaire de Dematologie Topographique Régionale. Paris 1905.
- Purvis DJ, et al: Gomez-Lopez-Hernandez syndrome: another consideration in focal congenital alopecia. The British journal of Dermatology 2007; 157: 196-198.









