
Background: Neuronitis vestibularis (VN) severely restricts affected individuals in their daily life. Typically, VN begins with severe and persistent dizziness, often accompanied by vomiting or nausea. The mechanisms and neurological substrates involved in the diverse subprocesses of vestibular compensation have not been fully explored. Because of the uncertainty about the pathophysiologic relationships, there is also controversy about the best possible treatment for unilateral VN. A common therapy is a one-week infusion of corticosteroids. In the acute phase, antiemetics such as dimenhydrinate, meclicin, or prochlorperazine are used to treat symptoms. Assuming that these drugs can influence the healing process due to their sedative effect, this therapy is often limited to the first days of the disease. The effects of fixed-combination therapy of dimenhydrinate and cinnarizine and over a prolonged period on dizziness in acute unilateral VN, were evaluated in a new study.
Question
In a patient population with vertigo in acute unilateral VN, what is the efficacy and tolerability of four weeks of treatment with the low-dose fixed combination 40 mg dimenhydrinate and 20 mg cinnarizine, administered with a standard corticosteroid infusion, compared with treatment with betahistine in terms of improvement in vertigo, its accompanying symptoms, and performance on neurootologic tests?
Inclusion criteria
- Treatment of acute unilateral VN.
- Age ≥18
- ≥1 of six vertigo symptoms (≥3 on a 10-cm visual analog scale [VAS], pathologic balance findings such as CDP [computerized dynamic posturography], and caloric testing [ENG]).
Exclusion criteria
- Hypersensitivity to the tested substances or to multiple drugs and limitations of the tested substances.
- Concurrent treatment with monoamine oxidase inhibitors, tricyclic antidepressants, parasympathetic agents, aminoglycoside antibiotics, anthistamines, or heparin.
- Taking glucocorticoids, antivertiginosa, and/or drugs with cerebrovascular activity other than those tested in the study.
Study design
Randomized, double-blind, active- and placebo-controlled parallel-group study, designed for non-inferiority, conducted at a single study site.
Study location
ENT Department of the University of Innsbruck in Austria.
Study groups
- Group 1: fixed combination of 20 mg cinnarizine and 40 mg dimenhydrinate
- Group 2: 12 mg betahistine three times daily
Eligible patients diagnosed with VN were randomly assigned to four weeks of treatment (28±2 days).
The drugs administered were indistinguishable from each other.
Measurement methods
Patients were examined before the start of medication, one week after (7± 2days) and four weeks after the start of the study (28±2 days) respectively.
The control examinations included:
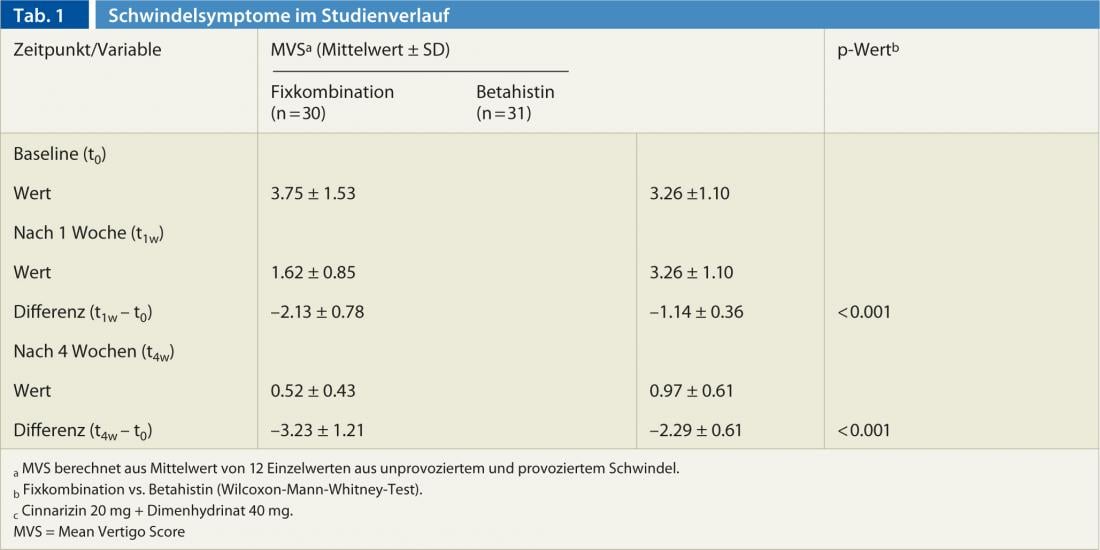
- Calculation of the mean vertigo score (MVS) based on the assessment of six (non-provoked) vertigo symptoms (standing and gait unsteadiness, staggering, spinning sensation, tendency to fall, feeling of lifting off, fainting) and dizziness triggered by six factors (change of position, leaning forward, standing up, traveling by car/train, head and eye movement) by patients on a visual, non-graded 10 cm analog scale.
- Assessment of the patients’ experienced impairment of ADL (activities of daily living) on a three-point scale by the subjects.
- Performance of a complete sensory organization test (SOT). Side effects and adverse events were queried and recorded on the examination days. Overall tolerability of treatment was rated as “very good,” “good,” “moderate,” or “poor” by patients and study physicians at one and four weeks after study entry.
Results
A total of 62 patients were randomized: Group 1 (fixed combination) n=30 and Group 2 (betahistine) n=32.
One patient from group 2 dropped out for unknown reasons before the end of the first week of the study.
Thus, the modified intent-to-treat population and the per-protocol population consisted of 61 patients.
Subjects in the two groups were comparable with respect to relevant baseline characteristics.
Effectiveness:
- The reduction in dizziness based on assessment with the MWS was significantly greater in group 1 than in the group of patients receiving betahistine (p<0.001). After four weeks, the dizziness symptom decreased by more than 85% in group 1 (fixed combination) and by 70% in group 2 (Table 1).
- Vegetative symptoms improved significantly more in group 1 (fixed combination) than in group 2.
- In addition, the fixed combination subject group showed statistical superiority over group 2 with respect to assessment of ADL: patients in group 1 rated their impairment of activities of daily living lower than patients in group 2.
Tolerability: None of the patients reported adverse events: Except for one patient (in group 2), tolerability was rated as very good or good at both study time points. After four weeks of treatment, 76.7% of patients on fixed-combination therapy found their tolerability to be very good, compared with 54.2% on betahistine.
Discussion
Due to the absence of a placebo group, the absolute efficacy of the medication in the study cannot be concluded for ethical reasons. However, the results found show that the improvement of vertigo symptoms and accompanying vegetative symptoms was significantly more pronounced in the fixed-combination patient group than in the betahistine-treated group. The results of the study, which was initially designed for non-inferiority, even showed superiority of the fixed combination after one and after four weeks of therapy. No significant side effects or adverse events occurred, with concomitant high tolerability rates in both patient groups.
The dizziness-reducing effect of the fixed combination can be attributed to the different actions of the two substances: on the one hand, the peripheral action due to the calcium antagonist cinnarizine, and on the other hand, the central action of dimenhydrinate, which regulates the activity of the vestibular nucleus and the adjacent autonomic center in the brainstem
Conclusions
The results of the study show that four weeks of treatment with the low-dose fixed combination 40 mg dimenhydrinate and 20 mg cinnarizine is an effective and well-tolerated treatment option for acute unilateral VN in a subject population of 61. The therapy had a significantly higher effect on improving dizziness and accompanying symptoms than treatment with betahistine, both after one week of treatment and after four weeks of therapy.
Literature:
- Scholtz, A, et al: Comparison of the Therapeutic Efficacy of a Fixed Low-Dose Combination of Cinnarizine and Dimenhydrinate with Betahistine in Vestibular Neuritis .Clin Drug Investig 2012; 32 (6): 387-399.









