Hyperthermia is a potent radio-sensitizer. The evidence base is good, especially for re-irradiation of tumor recurrences in pre-exposed areas. Thermal radiotherapy as part of primary curative therapy is currently being evaluated.
Hyperthermia (HT) can be considered the oldest form of cancer therapy. It was first used in 5000 BC. mentioned in traditions of the Egyptians [1] and later also in antiquity by Hippocrates. In the early 19th century, William Coley was able to achieve tumor regression in sarcoma patients by injecting bacterial lysates to produce sepsis with high fever (hyperthermia) [2]. He is considered the founder of cancer immunotherapy, although alternatively he can also be considered the first user of HT in modern times. In the 1980s, HT emerged in combination with radiotherapy (RT) but failed to gain acceptance due to misconceptions about heat application and lack of technical capabilities for controlled heat application [3]. In the last two decades, technical developments in heat application and its monitoring have made it possible to evaluate the effect of HT objectively and according to the principles of “evidence-based medicine”.
Basics
HT is an induced temperature elevation to 39-45°C in tumor tissue, with “mild temperature hyperthermia” (MTH) of 39-41°C over one to two hours most commonly applied clinically. Temperatures of >45°C are called thermoablation and have a different mechanism of action.
The heat application in the HT can be used both by
- externally in the form of regional surface hyperthermia (OHT) (for tumors up to 4 cm from the skin surface), regional deep hyperthermia (THT) (for tumors greater than 4 cm from the skin surface), MR-controlled partial body hyperthermia, or from
- interstitial or
- intracavitary.
Evidence-based hyperthermia is not used as cancer monotherapy, but in combination with RT or chemotherapy (ChT). The best data on this is in combination with RT. As shown in a cross-tumor meta-analysis of randomized and non-randomized studies, concurrent thermal radiotherapy (HTRT) leads to a 15% improvement in complete response (CR) compared to RT alone [4]. In breast carcinoma and chest wall recurrences even +22% [5], in ENT tumors +23% [6] and cervical carcinomas +23% [7] (significant in each case: p<0.0001 and p<0.001, respectively). Thus, the benefit of concurrent HTRT was documented, especially in locally advanced tumors, in terms of CR and thus improved local control.
How does hyperthermia work?
Tumor heating leads to enhancement of concurrently applied RT and/or ChT. Combined with the RT, the HT acts as a potent radio sensitizer [4,8–9]. It acts against cancer cells on several levels. HT leads to the improvement of tumor microperfusion through vasodilation, thus better oxygenating hypoxic and thus radioresistant tumor cells [10]. In combination with RT, this leads to increased DNA single and double strand breaks. Further, HT inhibits subsequent DNA repair mechanisms [11]. HT induces immune stimulation through increased expression of heat-shock proteins, which, via Natural Killer Cells and antigen-presenting dendritic cells, cause increased activation of CD8+ T lymphocytes and thus an immune system-mediated, specific antitumor response [12]. Thus, in addition to the local effect, HT can also have a systemic effect.
In which situations/tumor entities is hyperthermia applied?
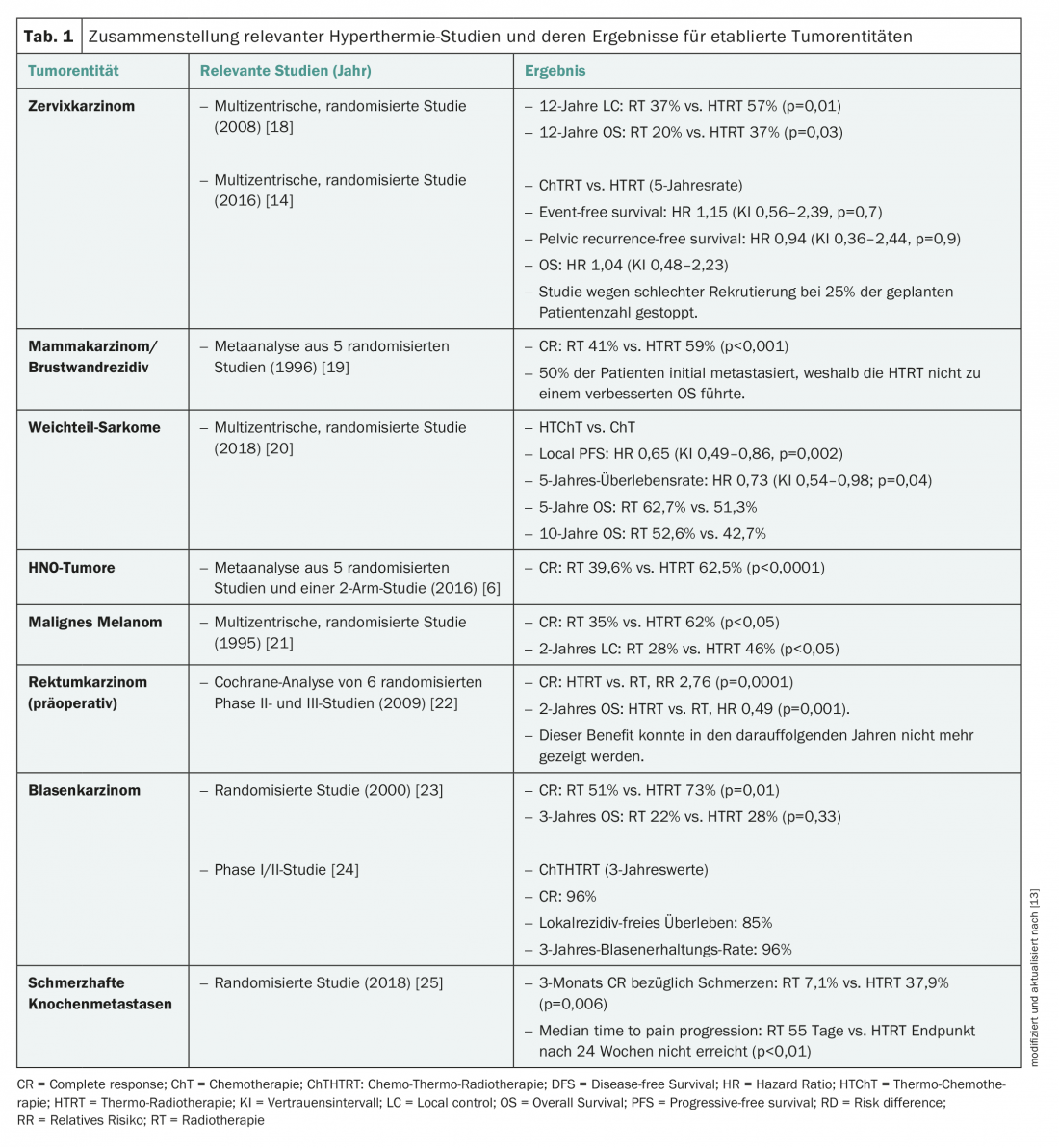
HT can theoretically be used in all tumor entities, if technically feasible. It is used in two areas of application: As a radio-sensitizer in re-irradiation (Re-RT) in pre-exposed tissue to save radiation dose or as a radio-sensitizer in primary treatments to increase the effectiveness of the applied radiation dose (Tab. 1) [4,9,13].
Re-irradiations: In the case of tumor recurrence in pre-irradiated areas, re-irradiation with a sufficient radiation dose can usually only be performed at the cost of radiation toxicities. Pre-irradiated tissue usually exhibits fibrosis with decreased perfusion. Heating with vasodilation and better microperfusion uniquely counteracts this. In addition, the other radiosensitizing properties mentioned above come into play. Thus, concomitant HT allows compensation for lower dose application. In this regard, local recurrence in breast carcinoma after adjuvant RT is the most common and also the best studied entity [5]. HTRT in this situation is listed as a “category 3 recommendation” in the NCCN Guidelines (NCCN Guidelines version 1.2018, MS-67).
Radio-sensitizers in primary treatments: Although positive randomized phase III trials and meta-analyses have been published in some tumor entities, HTRT is not listed as the gold standard in any tumor entity. On closer inspection, it is noticeable that the studies are mostly older and that HTRT was mostly compared with RT alone, which is no longer considered standard today. Typical examples include cervical, rectal, urinary bladder and ENT tumors. The initiation of new multicenter and international studies is hampered by the low density of European HT centers and, compared to the liaison between the pharmaceutical industry and medical oncology, by a lack of financial support. Thus, when HT is available, it is usually used as a radiosensitizing alternative in non-chemotherapy-naive patients.
Since correctly performed HT usually has no additional relevant toxicities [4], HTRT might be favored even in case of “non-inferiority” regarding outcome compared to radiochemotherapy (RTChT) due to fewer side effects. This direct comparison has been investigated in only a few studies [14]. Thus, efforts are underway to combine HT in curative primary treatment in trials either alone with RT or together with RTChT resp. ChT to be applied.
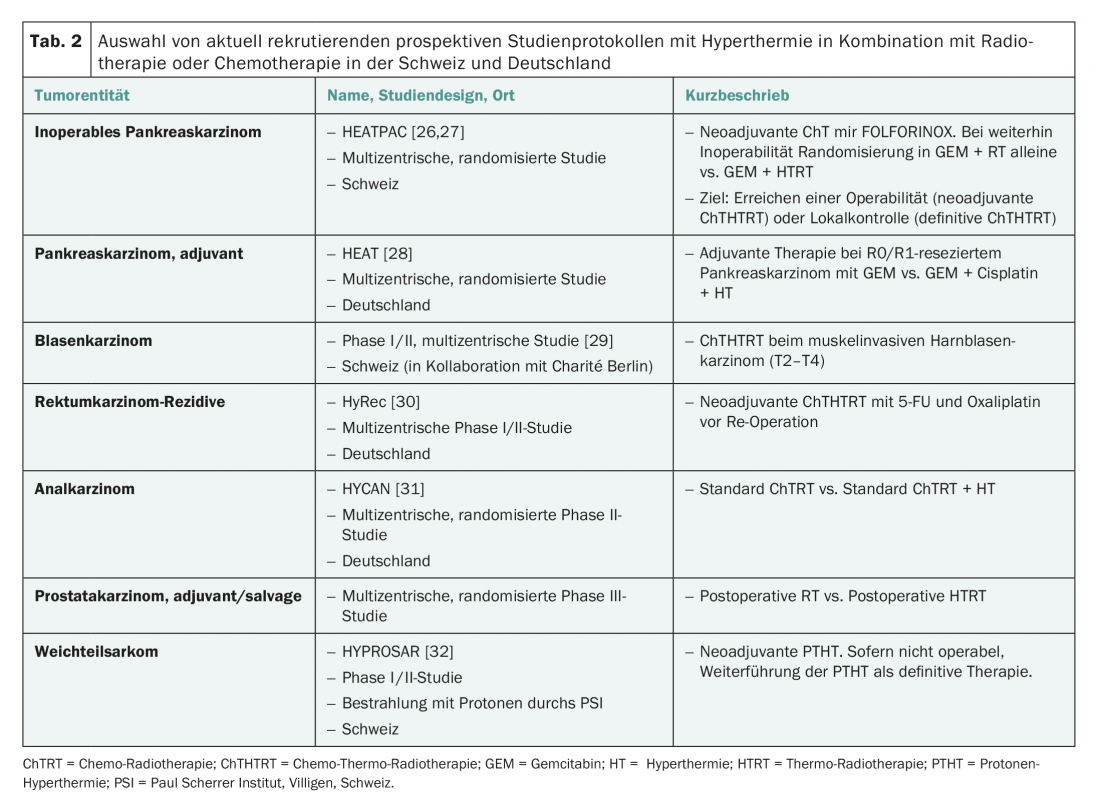
For overview purposes, a selection of currently recruiting study protocols with HT in Switzerland and Germany is summarized in Table 2.
Contraindications for hyperthermia
HT is not applicable to all patients. The painless positioning on the back and the application of heat must be ensured for about one and a half hours. be tolerable. Due to electromagnetic waves, ICD/pacemakers, along with metal prostheses and osteosynthesis material near the tumor area, are contraindications. The former may cause malfunction, the latter excessive local heating with burns. Further, not every tumor location qualifies for HT. From a technical point of view, the body region to be heated must be accessible to the HT applicator. For example, deep-seated tumors in the ENT region that are not accessible to OHT cannot be reached due to the ring-shaped applicator of THT. However, a special applicator [15] was developed for this purpose. Further, tumors surrounded by air (e.g., lung tumors) may be difficult to heat due to low thermal conduction.
How is hyperthermia applied?
HT is applied depending on the HT device and tumor location (OHT vs. THT). Once or twice a week, usually before radiotherapy, the tumor region is heated to a temperature of 41-43°C for 45-60 minutes.
In THT, planning computed tomography is performed in the HT (“hammock”) position prior to the first session, and the volume to be heated is drawn in analogously to the PTV (Planning Target Volume). Physical models can be used to calculate the temperature at the target site using calibrated algorithms (similar to calculating the planned radiation dose in tissue) or measured at body sites or orifices (skin surface, bladder, rectum, vagina, etc.) using indirect real-time thermometry. The heat supply is adjusted accordingly. The most accurate would be an interstitial temperature measurement in the tumor. However, the possibility of infection or implantation metastases makes this type of measurement an exception.
The OHT is comparatively simple. Again, interstitial temperature measurement is omitted. Thus, the measurement is made by means of temperature probes on the skin, and in real time the heat application can be controlled.
Hyperthermia in Switzerland
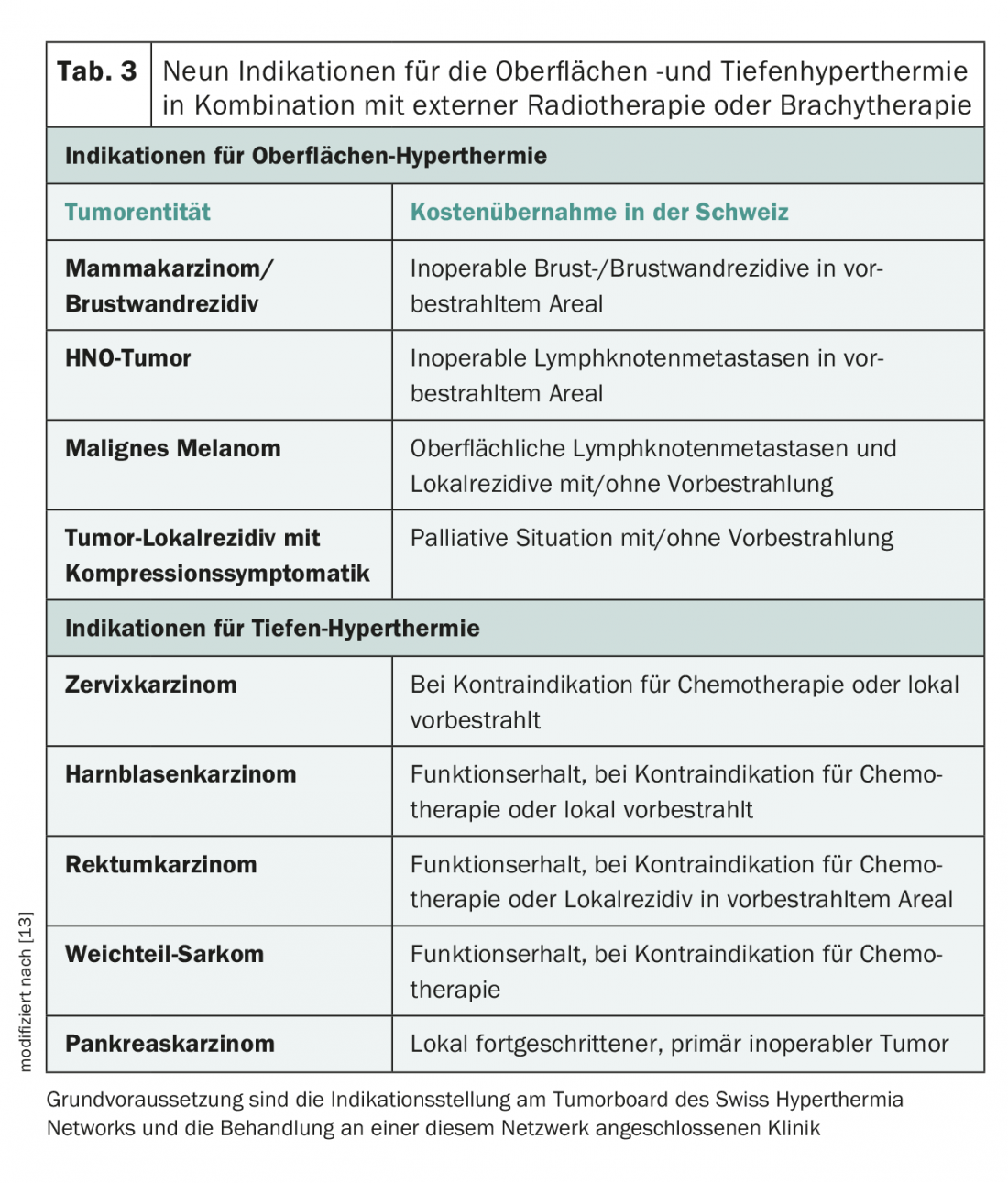
In Switzerland, HT is fully covered by health insurance for nine indications (Tab. 3) with simultaneous outpatient RT, provided that the patients are presented at the weekly virtual Swiss Hyperthermia Network Tumorboard (SHN) and the indication for HT was made within this framework. Since there are currently only a few HT centers in Switzerland (for THT only the Cantonal Hospital Aarau), good interinstitutional cooperation is necessary. The externally referred patient usually receives hyperthermia and radiation at the HT center one day per week. The remaining, usually 80%, of the radiation treatments are performed by the referring physician.
The Swiss Hyperthermia Network (SHN) coordinates further HT studies and innovative technical projects under the patronage of the Cantonal Hospital Aarau. For example, a new HT device is being developed in collaboration with ITIS/ETH Zurich [16]. For further information, please refer to the recently published article in the Swiss Cancer Bulletin [17].
Take-Home Messages
- Hyperthermia is a potent radio-sensitizer with a good evidence base, especially for re-irradiation of tumor recurrence in pre-exposed areas.
- Hyperthermia can be used as an alternative radio-sensitizer along with radiotherapy in non-chemotherapy patients in the curative setting.
- Thermal radiotherapy as part of primary curative therapies is being evaluated in ongoing trials.
Conflict of interest: The authors offer hyperthermia in combination with radiotherapy at the Cantonal Hospital Aarau. Together with Markus Notter, MD, Lindenhofspital Bern, they are founders of the Swiss Hyperthermia Network.
Acknowledgements: The authors would like to thank the following persons: Prof. Dr. med. Daniel Aebersold, University Department of Radio-Oncology, Inselspital Bern for the critical review of this article; the rest of the board of the Swiss Hyperthermia Network (SHN) namely Dr. med. Markus Notter (Lindenhofspital Bern), PD Dr. med. Günther Gruber (Hirslanden Klinik Zürich), Prof. Dr. med. Dr. med. Thomas Ruhstaller (Kantonsspital St. Gallen) and Prof. Dr. Nicolaus Andratschke (University Hospital Zurich); to the remaining working group “Hyperthermia” of the Radio-Oncology Center KSA-KSB, namely Dr. Gerd Lutters, Dietmar Marder, Olaf Timm and Prof. Stephan Scheidegger; to the Cancer League Aargau, the Research Council Kantonsspital Aarau, the Günter-und-Regine-Kelm-
Foundation and the Isler Fund for their many years of financial support.
Literature:
- Breasted JH: The Edwin Schmid surgical papyrus. In: Light S, editor. Therapeutic heat and coal. 2nd ed. Baltimore: Waverly Press 1930: 196.
- Coley WB: The treatment of malignant tumors by repeated inoculations of erysipelas, with a report of ten original cases. Am J Med Sci 1893; 105: 488-511.
- Dewhirst MW, et al: Re-setting the biologic rationale for thermal therapy. Int J Hyperthermia 2005; 21(8): 779-790.
- Datta NR, et al: Local hyperthermia combined with radiotherapy and-/or chemotherapy: recent advances and promises for the future. Cancer Treat Rev 2015; 41: 742-753.
- Datta NR, et al: Hyperthermia and Radiation Therapy in Locoregional Recurrent Breast Cancers: A Systematic Review and Meta-analysis. Int J Radiat Oncol Biol Phys 2016; 94: 1073-1087.
- Datta NR, et al: Hyperthermia and radiotherapy in the management of head and neck cancers: A systematic review and meta-analysis. Int J Hyperthermia 2016; 32: 31-40.
- Datta NR, et al: Hyperthermia and radiotherapy with or without chemotherapy in locally advanced cervical cancer: a systematic review with conventional and network meta-analyses. Int J Hyperthermia 2016; 32: 809-821.
- Overgaard J: The heat is (still) on – the past and future of hyperthermic radiation oncology. Radiother Oncol 2013; 109: 185-187.
- Peeken JC, et al: Integrating Hyperthermia into Modern Radiation Oncology: What Evidence Is Necessary? Front Oncol 2017; 7: 132.
- Vaupel PW, et al: Pathophysiological and vascular characteristics of tumours and their importance for hyperthermia: heterogeneity is the key issue. Int J Hyperthermia 2010; 26(3): 211-223.
- Oei AL, et al: Effects of hyperthermia on DNA repair pathways: one treatment to inhibit them all. Radiat Oncol 2015; 10: 165.
- Toraya-Brown S, et al: Local tumor hyperthermia as immunotherapy for metastatic cancer. Int J Hyperthermia 2014; 30(8): 531-539.
- Stutz E, et al: Value of regional hyperthermia in cancer therapy. Schweiz Med Forum 2017; 17(48): 1074-1076.
- Ludgens LC, et al: Radiation therapy combined with hyperthermia versus cisplatin for locally advanced cervical cancer: results of the randomized RADCHOC trial. Radiother Oncol 2016; 120(3): 378-382.
- Verduijn GM, et al: Deep hyperthermia with the HYPERcollar system combined with irradiation for advanced head and neck carcinoma – a feasibility study. Int J Hyperthermia 2018; 34(7): 994-1001.
- Dressel S, et al: Novel hyperthermia applicator system allows adaptive treatment planning: preliminary clinical results in tumor-bearing animals. Vet Comp Oncol 2018; 16: 202-213.
- Datta NR, et al: Swiss Hyperthermia Clinical and Research Activities: Integrating with Radiation Therapy. Swiss Cancer Bulletin 2018; 3: 249-252.
- Franckena M, et al: Long-term improvement in treatment outcome after radiotherapy and hyperthermia in locoregionally advanced cervix cancer: an update of the Dutch Deep Hyperthermia Trial. Int J Radiat Oncol Biol Phys 2008; 70: 1176-1182.
- Vernon CC, et al: Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: results from five randomized controlled trials. International Collaborative Hyperthermia Group. Int J Radiat Oncol Biol Phys 1996; 35: 731-744.
- Issels RD, et al: Effect of Neoadjuvant Chemotherapy Plus Regional Hyperthermia on Long-term Outcomes Among Patients With Localized High-Risk Soft Tissue Sarcoma: The EORTC 62961-ESHO 95 Randomized Clinical Trial. JAMA Oncol 2018; 4(4): 483-492.
- Overgaard J, et al: Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. European Society for Hyperthermic Oncology. Lancet 1995; 345: 540-543.
- De Haas-Kock DFM, et al: Concomitant hyperthermia and radiation therapy for treating locally advanced rectal cancer. Cochrane Database Syst Rev 2009; (3): CD006269.
- Van der Zee J, et al: Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: a prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. Lancet 2000; 355: 1119-1125.
- Wittlinger M, et al: Quadrimodal treatment of high-risk T1 and T2 bladder cancer: transurethral tumor resection followed by concurrent radiochemotherapy and regional deep hyperthermia. Radiother Oncol 2009; 93(2): 358-363.
- Chi MS, et al: Comparing the Effectiveness of Combined External Beam Radiation and Hyperthermia Versus External Beam Radiation Alone in Treating Patients With Painful Bony Metastases: A Phase 3 Prospective, Randomized, Controlled Trial. Int J Radiat Oncol Biol Phys 2018; 100(1): 78-87.
- ClinicalTrials.gov: https://clinicaltrials.gov/ct2/show/NCT02439593?term=heatpac&rank=1 [Accessed 19.09.2018]
- Datta NR, et al: “HEATPAC” – a phase II randomized study of concurrent thermochemoradiotherapy versus chemoradiotherapy alone in locally advanced pancreatic cancer. Radiat Oncol 2017; 12(1): 183.
- ClinicalTrials.gov: https://clinicaltrials.gov/ct2/show/NCT01077427?term=HEAT&cond=pancreatic+cancer&rank=5 [Accessed 19.09.2018]
- Datta NR, et al: Is hyperthermia combined with radiotherapy adequate in elderly patients with muscle-invasive bladder cancers? Thermo-radiobiological implications from an audit of initial results. Int J Hyperthermia 2016; 32: 390-397.
- ClinicalTrials.gov: https://clinicaltrials.gov/ct2/show/NCT01716949?term=hyrec&rank=1 [Accessed 19.09.2018]
- ClinicalTrials.gov: https://clinicaltrials.gov/ct2/show/NCT02369939?cond=anal+cancer+hyperthermia&rank=1 [Accessed 19.09.2018]
- Datta NR, et al: Proton irradiation with hyperthermia in unresectable soft tissue sarcoma. Int J Particle Ther 2016; 3: 327-336.
InFo ONCOLOGY & HEMATOLOGY 2018; 6(5): 35-39.