
The 38-year-old Marina T. from southern Italy has lived in Switzerland for 15 years without allergy problems. In summer, she travels with her husband by train from Zurich to Catanzaro in Calabria, her home town. During the last train journeys she regularly felt burning eyes during the short stop in Lugano, and during the longer stay in Chiasso sneezing and rhinorrhea were added. Continuing the journey south, the symptoms of rhinoconjunctivitis intensified, arriving in Florence she had to cough, in Rome she felt the first symptoms of shortness of breath with slight whistling. Once in Catanzaro, she had to be admitted to the emergency ward with status asthmaticus in each case.
After returning from Italy, the patient presents to the allergy ward at the University Hospital Zurich.
Allergological assessment: what’s behind it?
The patient’s medical history shows the typical symptoms of a respiratory allergy with itching of the eyes and nose, sneezing attacks, rhinorrhea and bronchial asthma up to status asthmaticus. Train travel with open windows in midsummer and strict seasonality suggest an allergen present in the outdoor air in the south, but less so an indoor allergen or a food consumed during the train trip.
Allergological clarification
Prick tests with routine inhalation allergens (Alyostal, Stallergènes Laboratoires) were consistently negative. Supplemental prick tests with Mediterranean pollen at a later time were negative for olive, cypress, and ragweed, and massively positive for glasswort (Parietaria) (++++).
Specific IgE (CAP, FEIA, Pharmacia Diagnostics, Uppsala, Sweden, now Thermo Fisher) were positive for Parietaria judeica and Parietaria officinalis class 3 (16 resp. 12 kU/l).
A methacholine provocation test, performed in winter, was negative.
Diagnosis
Rhinoconjunctivitis and bronchial asthma in monovalent inhalant allergy to Parietaria pollen.
Procedure
For the next summer trip to Italy, the patient was recommended a prophylactic therapy with an antihistamine (Zyrtec®) per os and inhalations with cromoglycate (Lomudal®), a mast cell protector, to be initiated the day before and continued during the entire vacation. She was also prescribed a metered-dose aerosol (bronchodilator). In winter, specific immunotherapy (SIT) was initiated with the semi-depot preparation Alutard® (ALK) containing 50% Parietaria judeica and 50% Parietaria officinalis.
Course
In the first year, SIT pre-seasonal could only reach the dose of 20 000 SQ. Under prophylactic therapy, the trip and stay in Calabria occurred for the first time with only mild rhinoconjunctivitis, but no cough or asthma. In the following years with a regular maintenance dose of SIT with 100,000 SQ, the patient remained asymptomatic.
Comment
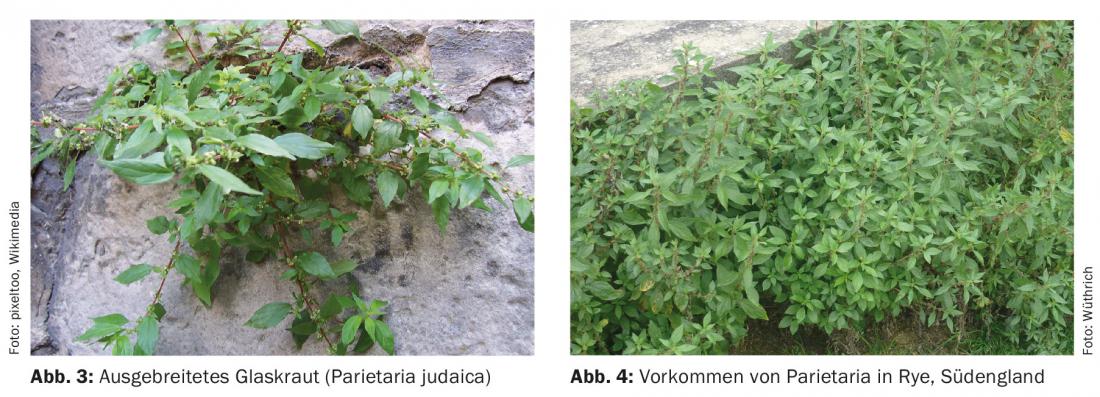
Glasswort (Parietaria) is a species of plant in the nettle family (Urticaceae). The botanical genus name Parietaria is derived from the Latin “paries” for “wall”, because this species often grows in walls (Fig. 1). The German name “Glaskraut” was given to the species of the genus because the herb used to be used for cleaning blind glasses and wine bottles (Fiaschi). Glasswort is a ruderal plant that grows on nutrient-rich soils, but also on rubble. There are two types of glasswort, Parietaria officinalis (upright glasswort, “pellitory-of-the-wall”, Fig. 2) and Parietaria judaica (spreading glasswort, “spreading pellitory”, Fig. 3) . The flowering period of Parietaria ranges from March to September/October, but basically the plants are able to flower all year round.

Glasswort is widespread in central and southern Europe and is introduced further north to southern England (Fig. 4) . In Germany, the main occurrences are in the Rhine valley and on the tributaries of the Rhine. In Switzerland, the spreading glasswort occurs more often on the southern side of the Alps in Ticino and Lake Geneva, as well as in South Tyrol. In South Tyrol, for example, the plant continues to spread and, as a wind-flowered species, it is now a feared allergy plant there.
Nothing is known about the prevalence of symptomatic parietaria pollinosis in Ticino. In a 1990 study of 110 pollinosis patients in an allergo-dermatology practice in Locarno, the frequency of sensitization to Parietaria officinalis was 17.3%, to Parietaria judaica 5.3% [1]. As a comparison, sensitization to grasses was found to be 66.7% and to birch 42.7% of pollen-allergic patients. In another larger study of 503 consecutive patients (57% male, 43% female) with pollinosis who visited the same practice in Locarno between 1990 and 1993, sensitization to P. officinalis was 17.9% and to P. judaica 9.5%, as in the previous study [2]. In a study conducted by the Allergy Station Zurich in 1987, no sensitizations to Parietaria pollen were found.
However, in Mediterranean countries, parietaria pollen is one of the most common pollinosis triggers. They are 12-17 µm wide in diameter. However, in the microscopic preparation used to determine the pollen calendar of a region, pollen of Parietaria is indistinguishable from that of nettles, both Urticaceae. However, pollen from stinging nettles are weak allergens and are of little importance as pollinosis agents in Switzerland. The high sensitization rate among pollen allergy sufferers in the Mediterranean region and the fact that the symptoms, especially asthma, persist stubbornly into the winter and hyposensitization only leads to moderate success with great difficulty speak for a high sensitization potency of Parietaria pollen.
From the month of June, more than 500 pollen grains/m3 can be registered in the air in the Mediterranean area. There is a high homology between the allergens from Parietaria officinalis and Parietaria judaica. The same antigen community includes the stinging nettles, the mulberry trees and possibly also the elms due to the family relationships. Genetic studies indicate a high affinity of the major allergen to HLA-DR 5. The leaves and stems also have some allergenic potency. Parietaria pollinosis is of particular importance for patients who are in the Mediterranean area during the flowering season, as they are much more exposed there.
The major allergen of Parietaria officinalis is par o I, MG 14,000; of Parietaria judaica par j 1 , MG 10-13,000. Both belong to the non-specific lipid transfer protein family. In Parietaria judaica, the allergens Par j 2, also a “lipid transfer protein”, Par j 3, a profilin, and a Par j “calcium-binding protein” were still characterized. In the IgE-CAP test (Thermo Fisher), whole pollen extracts are determined as w19 (P. officinalis) and W21 (P. judaica), and as recombinant major allergen of P. judaica w211 (rPar j 2 ; LTP) [3–5].
Literature:
- Torricelli R, Gilardi S, Wüthrich B: Contributo epidemiologico sulle sensibilizzazioni ai pollini in pazienti pollinotici nel Canton Ticino. Tribuna Medica Ticinese 1991; 56: 227-228.
- Gilardi S, et al: Pollinosis in the canton of Ticino. A prospective study in Locarno 1990-1993. Schweiz Med Wochenschr 1994; 124: 1841-1847.
- Cvitanović S: Allergy to Parietaria officinalis pollen. Croat Med J 1999; 40: 42-48.
- Colombo P, et al: The allergens of Parietaria. Int Arch Allergy Immunol 2003; 130: 173-179.
- Asturias JA, et al: Par j 1 and Par j 2, the major allergens from Parietaria judaica pollen, have similar immunoglobulin E epitopes. Clin Exp Allergy 2003; 33: 518-524.
DERMATOLOGIE PRAXIS 2015; 25(4): 29-31
DERMATOLOGIE PRAXIS 2018 Special Edition (Anniversary Issue), Prof. Brunello Wüthrich









