
Abdominal pain may be due to various pathological changes. Various diagnostic methods are used in the clarification process. Imaging techniques are particularly useful for confirming or excluding suspected diagnoses and for differential diagnostic purposes.
In recent months, imaging articles have presented numerous differential diagnoses of dysphagia. Now, abdominal pain will be the focus of upcoming publications. Numerous pathological changes are distinguished. Central position in the clarification of the causes of abdominal pain have history, laboratory and especially clinical examination [1–4].
Imaging techniques find their importance in the confirmation or exclusion of suspected diagnoses and in the differential diagnosis. The choice of imaging is influenced by the suspected diagnosis and question. In this context, it is important for the radiologist to obtain information on the patient’s medical history, current symptoms, relevant laboratory values (also with regard to contraindications to the administration of contrast media: hyperthyroidism and renal insufficiency, known contrast media intolerances) and suspected diagnosis.
The present article is intended to demonstrate exemplarily various pathological changes diagnosed by different methods. However, the situation is encountered in everyday clinical practice that a procedure does not yet clearly lead to a diagnosis. Sometimes a follow-up examination results in order to confirm a suspected diagnosis or to compensate, for example, for unfavorable sonographic conditions on abdominal ultrasonography in meteorism by computed tomography.
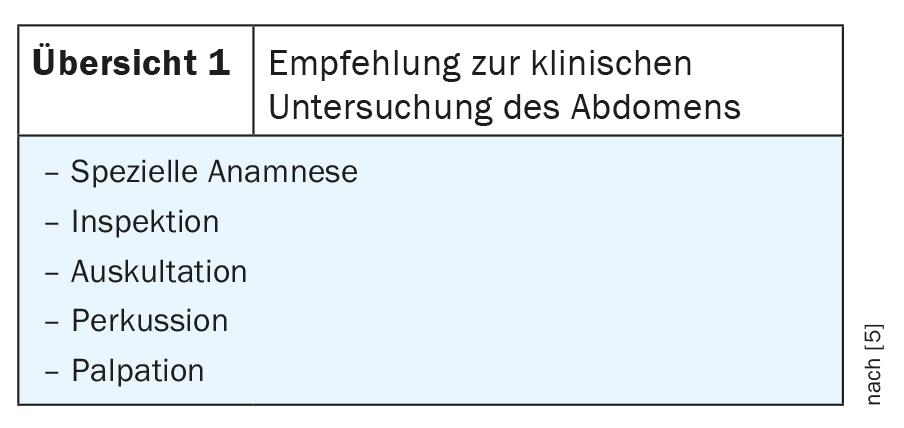
For clinical examination in abdominal symptomatology, the recommendation presented in review 1 is given [5].
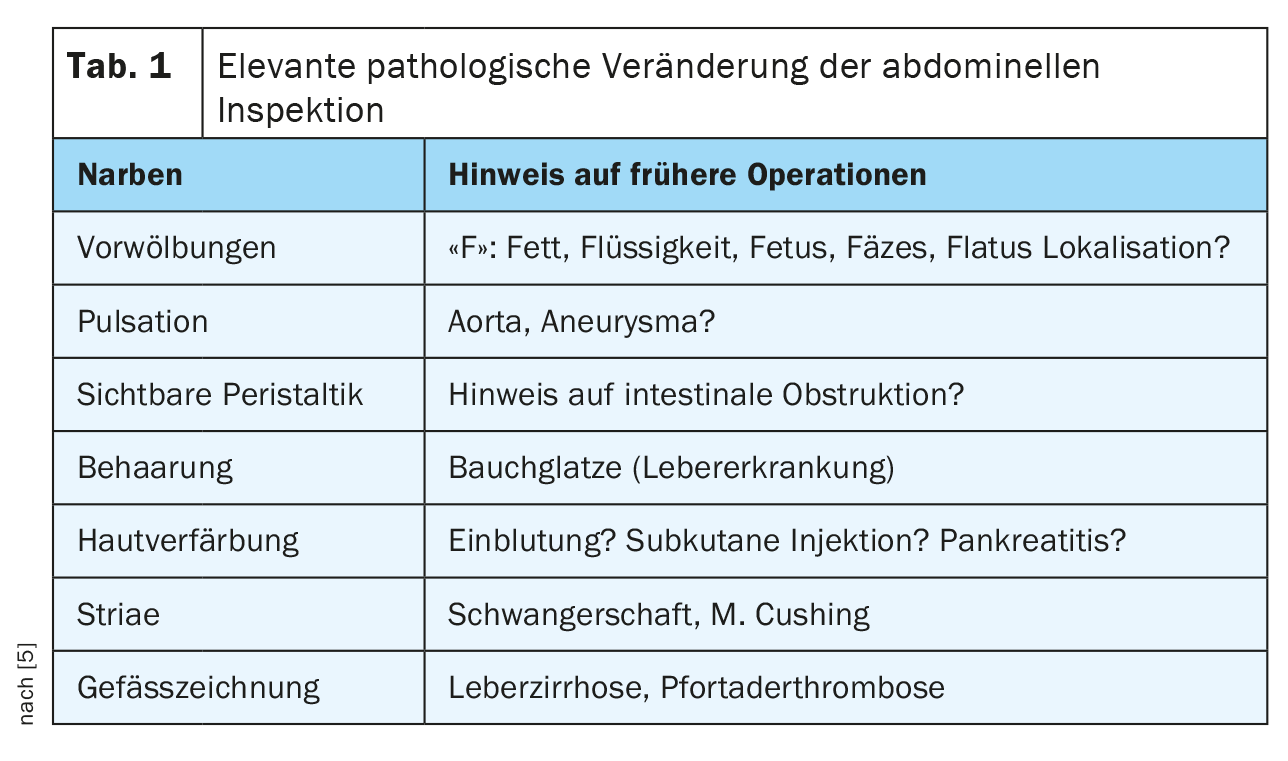
Even inspection can provide important information about the disease (Table 1).
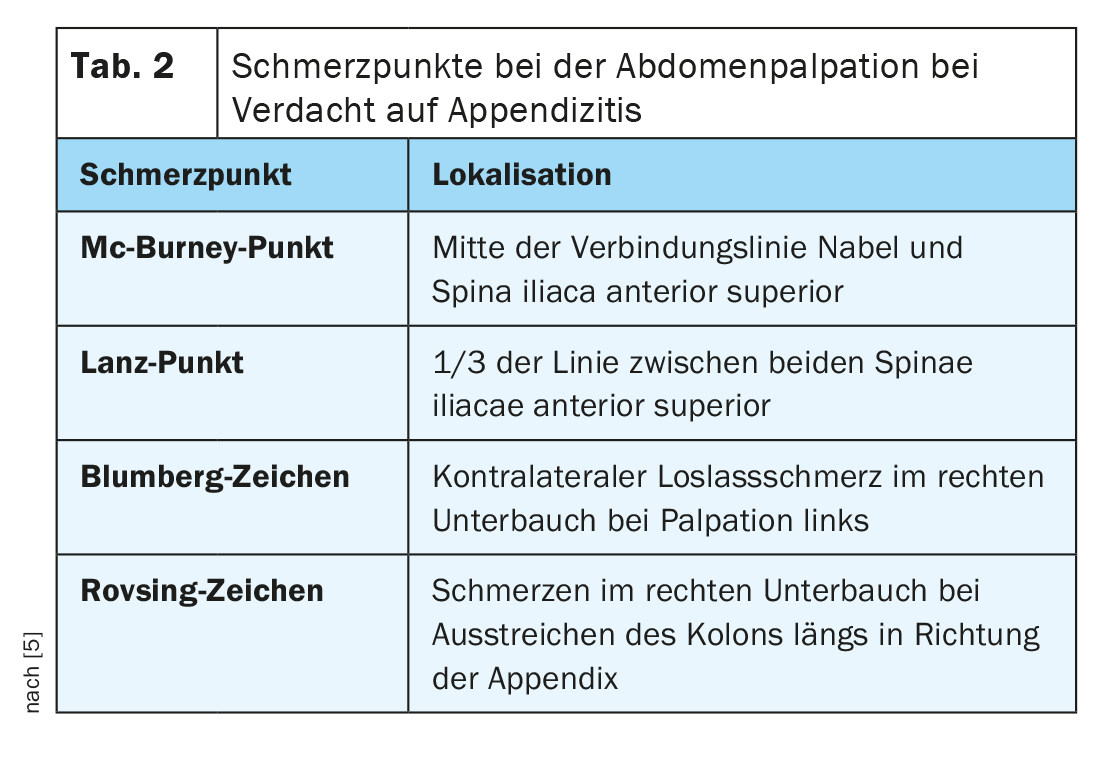
Finally, auscultation (indications of mechanical or paralytic ileus or increased peristalsis) or typical pain provocations (tab. 2) are also important during palpation. This can be very important in appendicitis, for example.
The geographic division of the abdomen and pelvis into right and left upper abdomen, middle and lower abdomen, and the regio umbilicalis is usually sufficient for initial orientation with the associated organs [2]. Approximately 5-10% of all patients presenting to emergency departments complain of acute abdominal pain [3].
Radiographs, with an abdominal view (in the standing or lateral position), may provide evidence of intestinal transit dysfunction (subileus, ileus) or suspect gastrointestinal perforation with free air. From a corresponding size and little overlay with intestinal air and contents, calcified concretions of the gallbladder or kidneys are recognizable, and in the case of metallic material used (vascular clips, forklift suture) also postoperative sequelae. Shadowing foreign bodies can be localized, traumatic changes of the local skeletal system can be detected.
Depending on the problem, computed tomographic examinations can be performed without intravenous contrast medium administration (e.g., stone search in the urinary system) or with (inflammatory or tumorous diseases). For radiation exposure, MRI should be favored as an alternative examination in young patients.
Magnetic resonance imaging can be used to verify inflammatory or tumorous changes in the abdominal region very well, especially with contrast-enhanced sequences. The corresponding contraindications must be observed.
Case studies
The case studies described here are exemplary for various pathological changes.
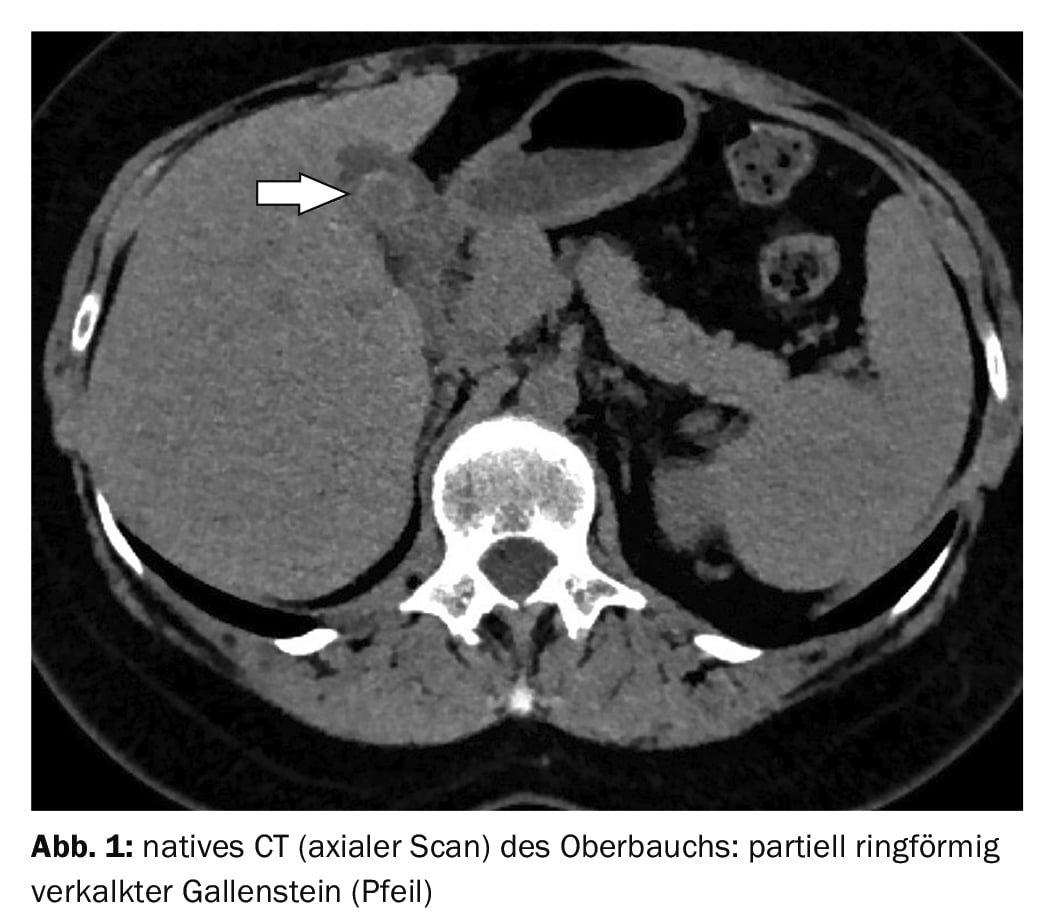
Case report 1 shows an annular calcified gallstone in a native CT scan of a 43-year-old female patient (Fig. 1) . There was recurrent pain under the right costal arch.
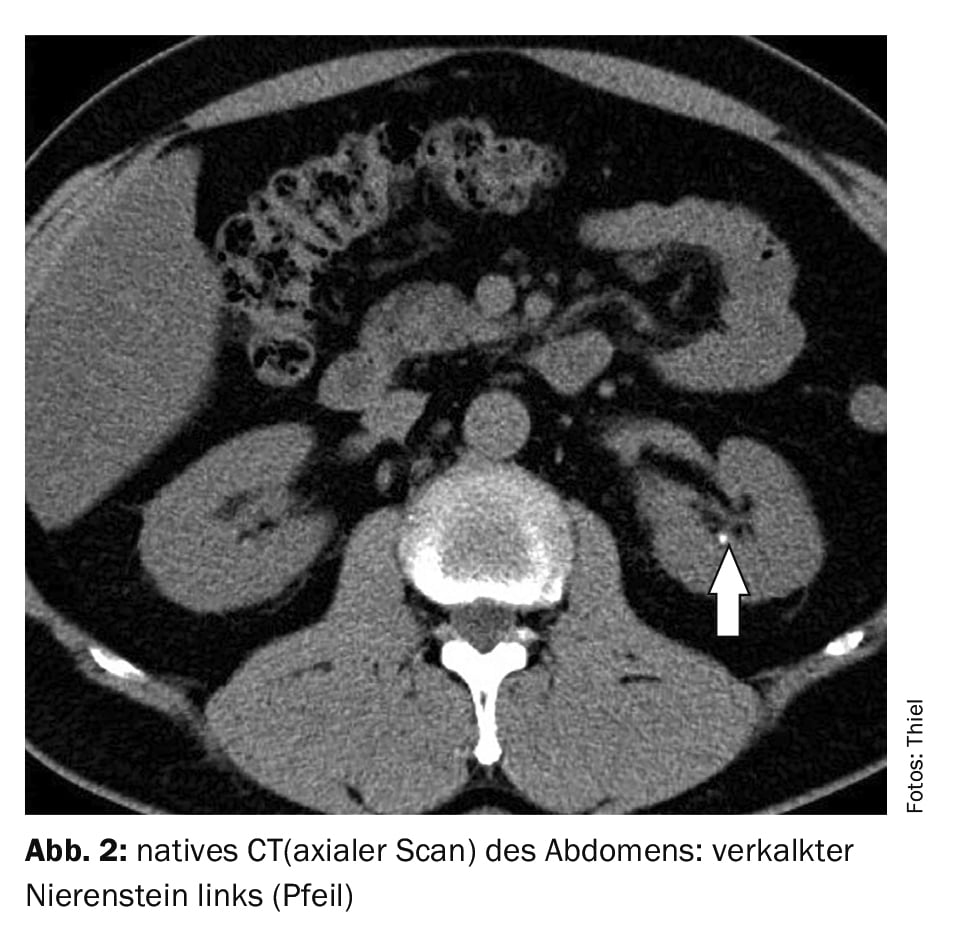
Case report 2 documents a calcified renal stone (Fig. 2) on native CT in a 58-year-old patient with renal colic.
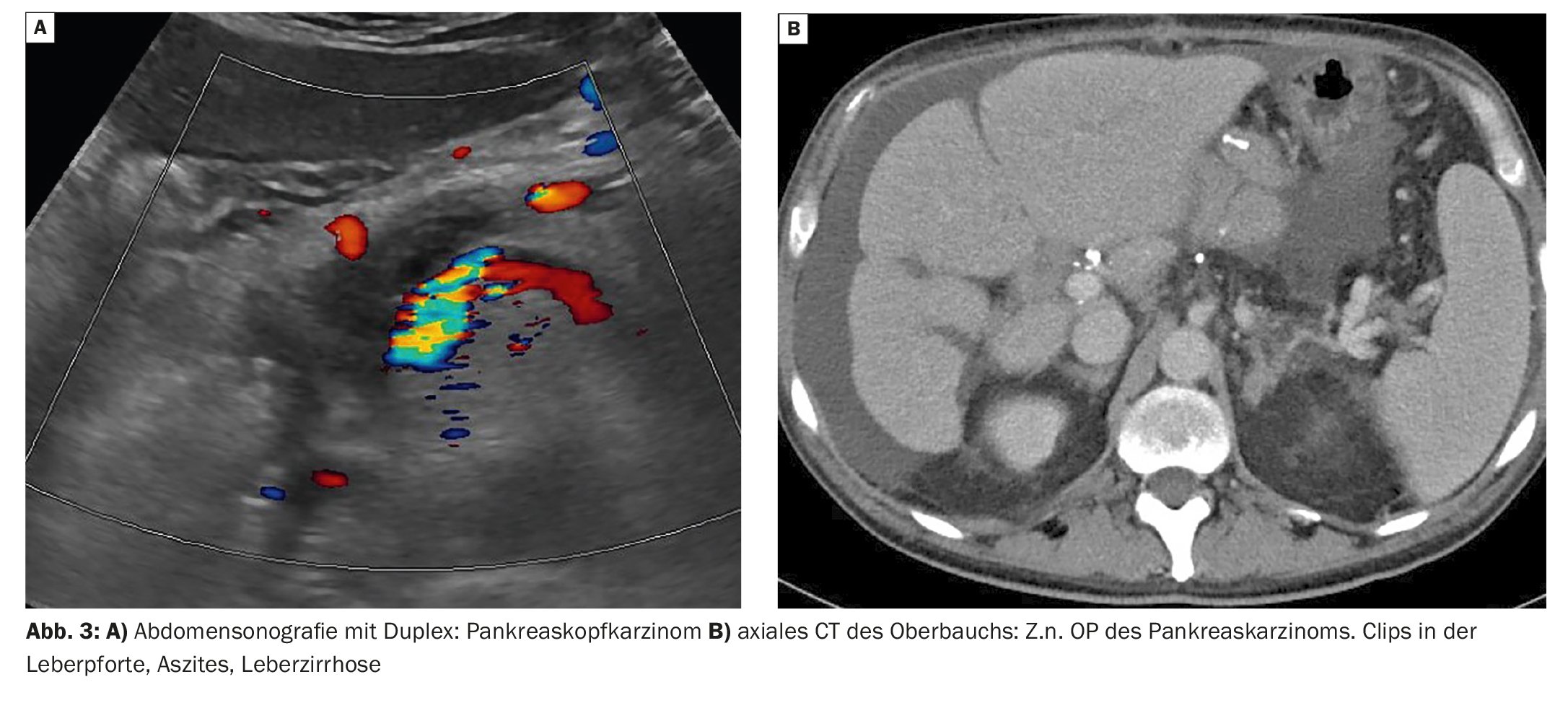
In case report 3, transverse ultrasound of the upper abdomen with duplex sonographically demonstrates carcinoma of the pancreatic head (Fig. 3A) in a 53-year-old man. The postoperative condition is shown in Figure 3B with ascites in liver cirrhosis.
Case report 4 shows terminal iliitis in a 23-year-old female patient with recurrent pain in the right lower abdomen (Fig. 4). MR sellink showed local wall inflammation and stenosis.

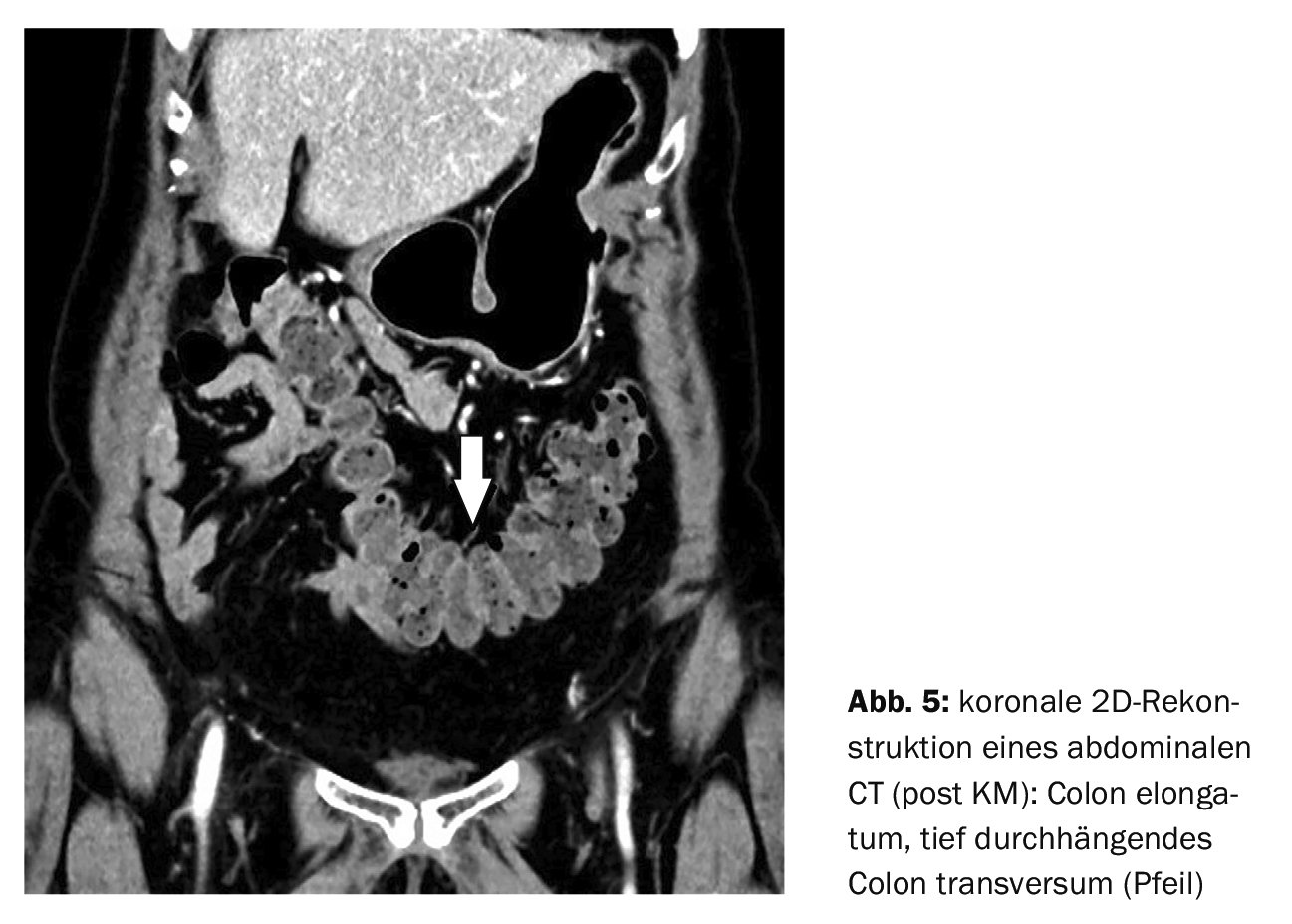
Recurrent diffuse abdominal pain and irregular bowel movements led a 49-year-old female patient to undergo computed tomography (case report 5), which demonstrated colonic elongation with a deeply sagging transversum (Fig. 5) . Probably a functionally related symptomatology resulted.
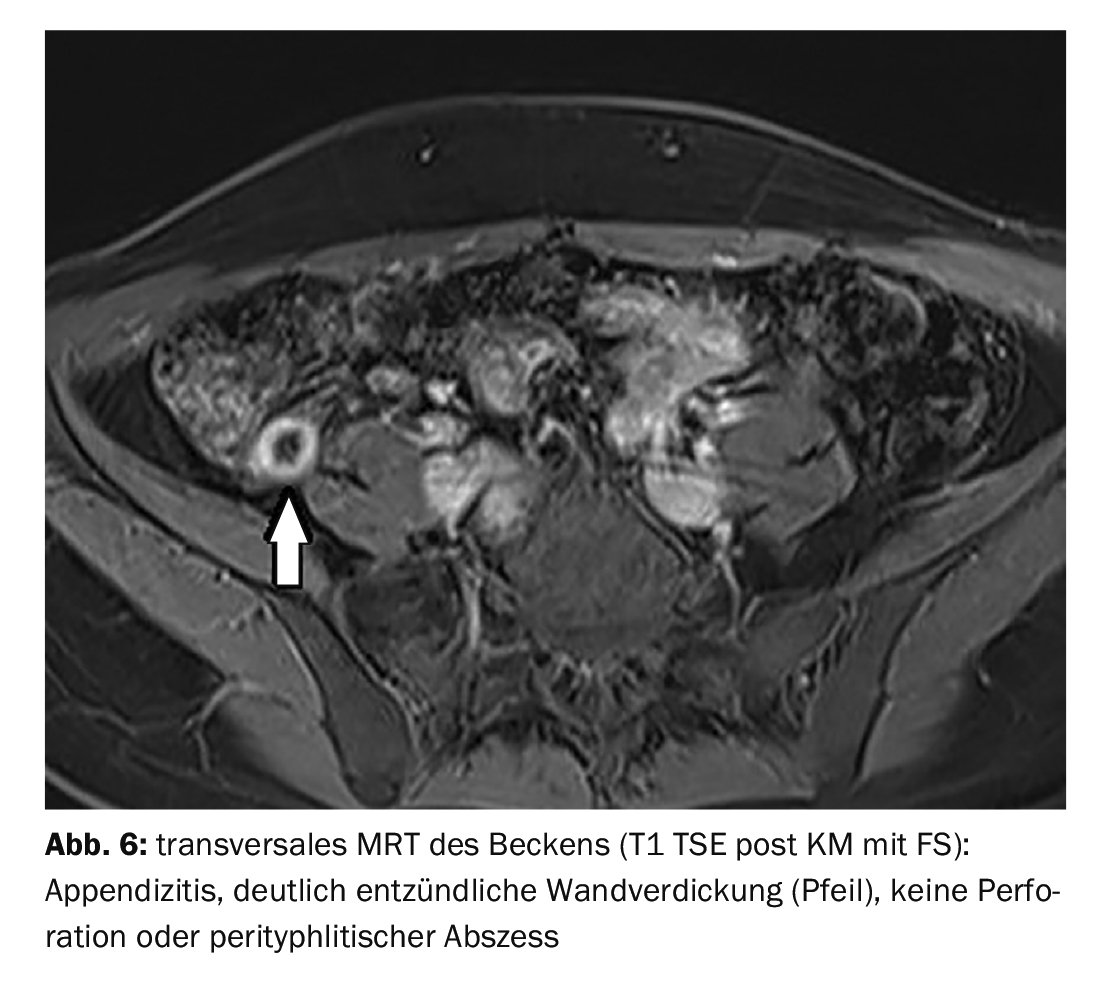
Case report 6 demonstrates acute appendicitis in a 22-year-old female patient with recurrent right lower abdominal pain (Fig. 6) . She had subfebrile temperatures, and laboratory and clinical examination were not suggestive. MR diagnosis was confirmed by surgery performed immediately after imaging.
Take-Home Messages
- A variety of parenchymatous and hollow organs are present in the abdomen and pelvis.
- Pain can be an expression of inflammatory or tumorous changes, a functional disorder, postoperative or traumatic lesions.
- Medical history, clinical and laboratory examination are important and usually directional.
- Imaging techniques support differential diagnosis and diagnosis finding
- In this context, the transmission of the previous examination results and a targeted questioning are enormously important for the radiologist.
Literature:
- Güller U, Macpherson AJ: Abdominal pain – differential diagnoses and diagnostic strategies in patients with chronic symptoms. Ther Umsch 2011; 68(8): 459-462.
- medizin kompakt: Bauch (Abdomen), www.medizin-kompakt.de/bauch-abdomen (last accessed 17.01.2023)
- Natesan S, Lee J, Volkamer H, Thoureen T: Evidence-Based Medicine Approach to Abdominal Pain. Emerg Med Clin North Am 2016; 34(2): 165-190.
- Sabo CM, Grad S, Dumitrascu DL: Chronic Abdominal Pain in General Practice. Dig Dis 2021; 39(6): 606-614.
- Füeßl H, Middeke M (Hrsg) Duale Reihe. Anamnese und Klinische Untersuchung, Untersuchung des Abdomens, 4. Auflage. Stuttgart: 2010.
HAUSARZT PRAXIS 2023; 18(3): 41–43









